

Adult venovenous extracorporeal membrane oxygenation for severe respiratory failure: Current status and future perspectives
- PMID: 26750681
- PMCID: PMC4900379
- DOI: 10.4103/0971-9784.173027
Adult venovenous extracorporeal membrane oxygenation for severe respiratory failure: Current status and future perspectives
Abstract
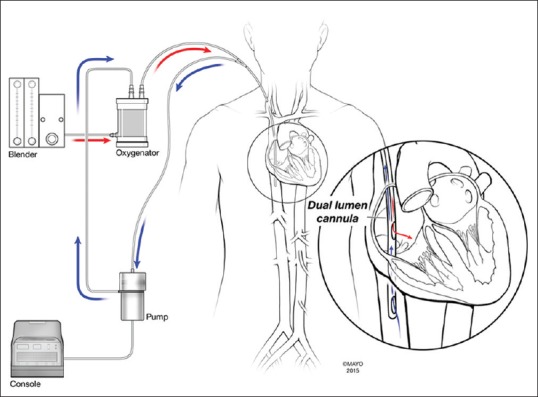
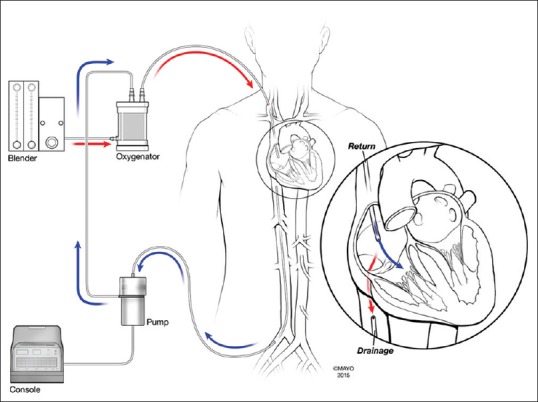
Extracorporeal membrane oxygenation (ECMO) for severe acute respiratory failure was proposed more than 40 years ago. Despite the publication of the ARDSNet study and adoption of lung protective ventilation, the mortality for acute respiratory failure due to acute respiratory distress syndrome has continued to remain high. This technology has evolved over the past couple of decades and has been noted to be safe and successful, especially during the worldwide H1N1 influenza pandemic with good survival rates. The primary indications for ECMO in acute respiratory failure include severe refractory hypoxemic and hypercarbic respiratory failure in spite of maximum lung protective ventilatory support. Various triage criteria have been described and published. Contraindications exist when application of ECMO may be futile or technically impossible. Knowledge and appreciation of the circuit, cannulae, and the physiology of gas exchange with ECMO are necessary to ensure lung rest, efficiency of oxygenation, and ventilation as well as troubleshooting problems. Anticoagulation is a major concern with ECMO, and the evidence is evolving with respect to diagnostic testing and use of anticoagulants. Clinical management of the patient includes comprehensive critical care addressing sedation and neurologic issues, ensuring lung recruitment, diuresis, early enteral nutrition, treatment and surveillance of infections, and multisystem organ support. Newer technology that delinks oxygenation and ventilation by extracorporeal carbon dioxide removal may lead to ultra-lung protective ventilation, avoidance of endotracheal intubation in some situations, and ambulatory therapies as a bridge to lung transplantation. Risks, complications, and long-term outcomes and resources need to be considered and weighed in before widespread application. Ethical challenges are a reality and a multidisciplinary approach that should be adopted for every case in consideration.
Figures
References
-
- Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000;342:1301–8. - PubMed
-
- Villar J, Blanco J, Añón JM, Santos-Bouza A, Blanch L, Ambrós A, et al. The ALIEN study: Incidence and outcome of acute respiratory distress syndrome in the era of lung protective ventilation. Intensive Care Med. 2011;37:1932–41. - PubMed
-
- Meade MO, Cook DJ, Guyatt GH, Slutsky AS, Arabi YM, Cooper DJ, et al. Ventilation strategy using low tidal volumes, recruitment maneuvers, and high positive end-expiratory pressure for acute lung injury and acute respiratory distress syndrome: A randomized controlled trial. JAMA. 2008;299:637–45. - PubMed
-
- Papazian L, Forel JM, Gacouin A, Penot-Ragon C, Perrin G, Loundou A, et al. Neuromuscular blockers in early acute respiratory distress syndrome. N Engl J Med. 2010;363:1107–16. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous