

Cluster-Randomized Non-Inferiority Trial to Compare Supplement Consumption and Adherence to Different Dosing Regimens for Antenatal Calcium and Iron-Folic Acid Supplementation to Prevent Preeclampsia and Anaemia: Rationale and Design of the Micronutrient Initiative Study
- PMID: 26751372
- PMCID: PMC4693340
- DOI: 10.4081/jphr.2015.582
Cluster-Randomized Non-Inferiority Trial to Compare Supplement Consumption and Adherence to Different Dosing Regimens for Antenatal Calcium and Iron-Folic Acid Supplementation to Prevent Preeclampsia and Anaemia: Rationale and Design of the Micronutrient Initiative Study
Abstract
Background: To prevent pre-eclampsia in populations with insufficient dietary calcium (Ca) intake, the World Health Organisation (WHO) recommends routine Ca supplementation during antenatal care (ANC). WHO guidelines suggest a complex dosing regimen, requiring as many as 5 pill-taking events per day when combined with iron and folic acid (IFA) supplements. Poor adherence may undermine public health effectiveness, so simpler regimens may be preferable. This trial will compare the effect of the WHO-recommended (higher-dose) regimen vs. a simpler, lower-dose regimen on supplement consumption and pill-taking behaviours in Kenyan ANC clients.
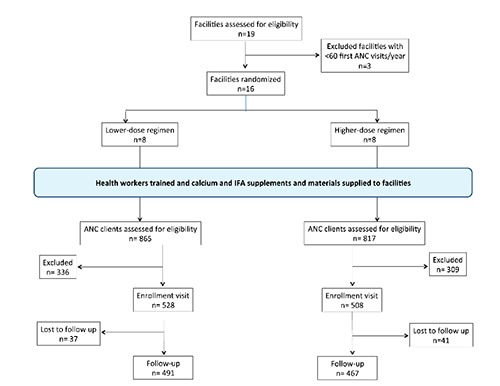
Design and methods: This is a parallel, non-inferiority, cluster-randomized trial; we examined 16 primary care health facilities in Kenya, 1047 pregnant women between 16-30 weeks gestational age. Higher-dose regimen: 1.5 g elemental calcium in 3 separate doses (500 mg Ca/pill) and IFA (60 mg Fe + 400 µg folic acid) taken with evening dose. Lower-dose regimen: 1.0 g calcium in 2 separate doses (500 mg Ca/pill) with IFA taken as above.
Measurements: Primary outcome is Ca pills consumed per day, measured by pill counts. Secondary outcomes include IFA pills consumed per day, client knowledge, motivation, social support, and satisfaction, measured at 4 to 10 weeks post-enrolment.
Statistical analyses: Unit of randomization is the healthcare facility; unit of analysis is individual client. Intent-to-treat analysis will be implemented with multi-level models to account for clustering.
Expected public health impact: If pregnant women prescribed lower doses of Ca ingest as many pills as women prescribed the WHO-recommended regimen, developing a lower-dose recommendation for antenatal Ca and IFA supplementation programs could save resources. Significance for public healthPre-eclampsia is a leading cause of maternal mortality. Based on clinical evidence of significant reduction in risk of pre-eclampsia, the WHO recommends including calcium (Ca) supplementation in antenatal care services in settings with inadequate dietary Ca intakes. A high daily amount of Ca administered in a complex dosing regimen is recommended to maximize efficacy and bioavailability. Factors such as client adherence, motivation, cost and logistical complexities may undermine effectiveness when implemented in public health programs. This cluster-randomized trial will compare Ca supplement consumption between higher and lower-dose regimens delivered through antenatal care in Kenya, integrated with iron-folic acid supplementation. If a lower-dose regimen improves adherence, women's Ca supplement consumption may be comparable to that achieved under a complex, higher-dose regimen. Evidence gained from this trial will guide public health planning for antenatal calcium supplementation programs to maximize benefits through reducing logistical, cost and adherence barriers.
Keywords: Preeclampsia; adherence; anaemia; calcium supplements; iron-folic acid.
Conflict of interest statement
Conflict of interest: the authors declare no potential conflict of interest.
Figures
References
-
- Cheng MH, Wang PH. Placentation abnormalities in the pathophysiology of preeclampsia. Expert Rev Mol Diagn 2008;9:37-49. - PubMed
-
- Cudihy D, Lee RV. The pathophysiology of pre-eclampsia: Current clinical concepts. J Obstet Gynaecol 2009;29:576-82. - PubMed
-
- Hofmeyr GJ, Duley L, Atallah A. Dietary calcium supplementation for prevention of pre-eclampsia and related problems: a systematic review and commentary. Int Gynaecol Obstet 2007;114:933-43. - PubMed
-
- Buppasiri P, Lumbiganon P, Thinkhamrop J, et al. Calcium supplementation (other than for preventing or treating hypertension) for improving pregnancy and infant outcomes. Cochrane Database Syst Rev 2011:CD007079. - PubMed
-
- World Health Organization. Guideline: calcium supplementation in pregnant women. Geneva: World Health Organization; 2013. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
