

A Probabilistic Atlas of Diffuse WHO Grade II Glioma Locations in the Brain
- PMID: 26751577
- PMCID: PMC4709135
- DOI: 10.1371/journal.pone.0144200
A Probabilistic Atlas of Diffuse WHO Grade II Glioma Locations in the Brain
Abstract
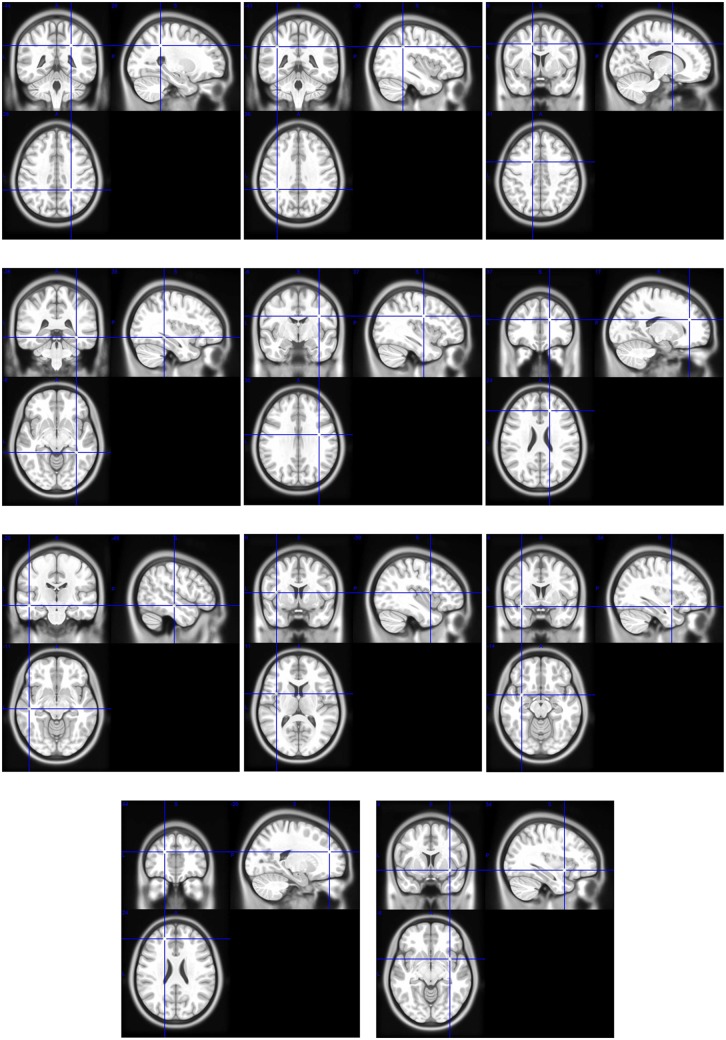
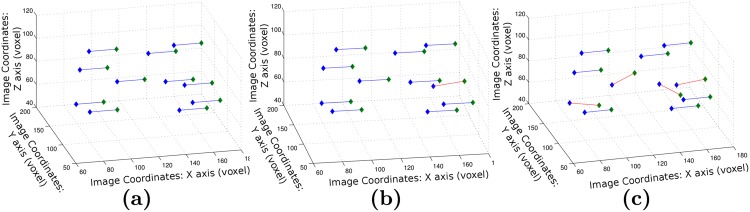
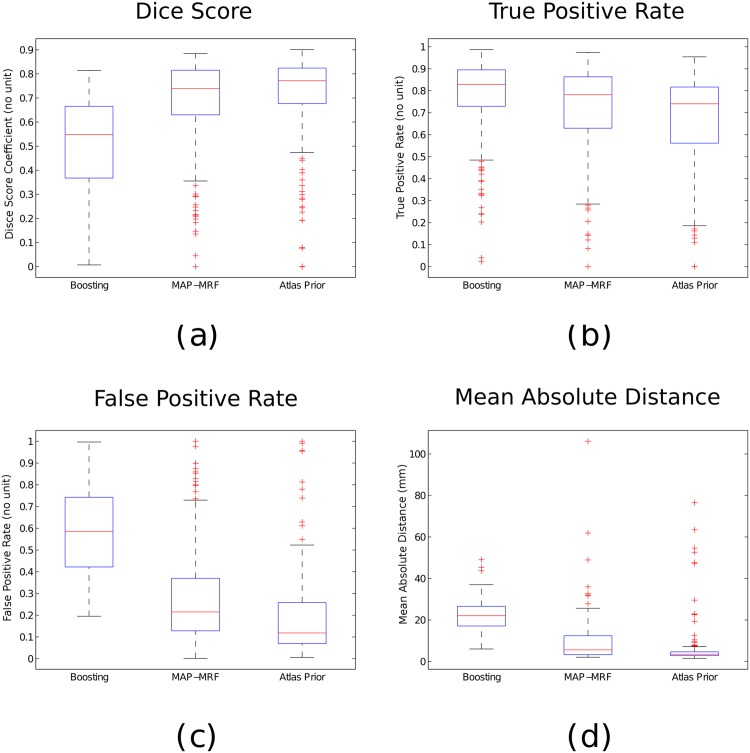
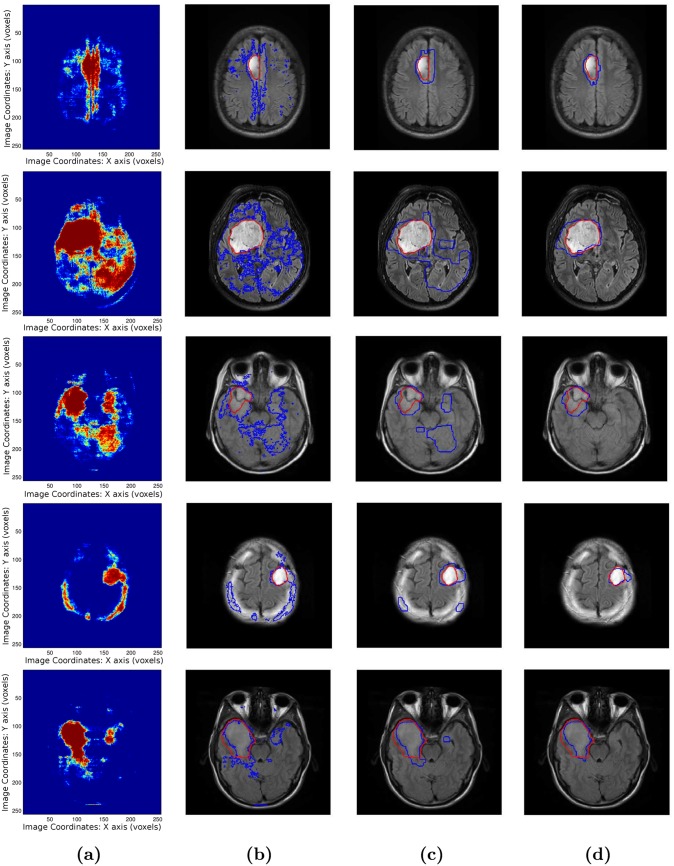
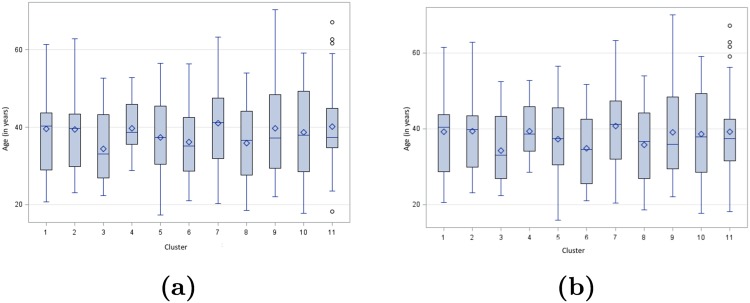
Diffuse WHO grade II gliomas are diffusively infiltrative brain tumors characterized by an unavoidable anaplastic transformation. Their management is strongly dependent on their location in the brain due to interactions with functional regions and potential differences in molecular biology. In this paper, we present the construction of a probabilistic atlas mapping the preferential locations of diffuse WHO grade II gliomas in the brain. This is carried out through a sparse graph whose nodes correspond to clusters of tumors clustered together based on their spatial proximity. The interest of such an atlas is illustrated via two applications. The first one correlates tumor location with the patient's age via a statistical analysis, highlighting the interest of the atlas for studying the origins and behavior of the tumors. The second exploits the fact that the tumors have preferential locations for automatic segmentation. Through a coupled decomposed Markov Random Field model, the atlas guides the segmentation process, and characterizes which preferential location the tumor belongs to and consequently which behavior it could be associated to. Leave-one-out cross validation experiments on a large database highlight the robustness of the graph, and yield promising segmentation results.
Conflict of interest statement
Figures
References
-
- Capelle L, Fontaine D, Mandonnet E, Taillandier L, Golmard JL, et al. (2013) Spontaneous and therapeutic prognostic factors in adult hemispheric world health organization grade ii gliomas: a series of 1097 cases: Clinical article. Journal of Neurosurgery 118: 1157–1168. 10.3171/2013.1.JNS121 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
