

Pharmacologic Interventions in Preventing Ovarian Hyperstimulation Syndrome: A Systematic Review and Network Meta-Analysis
- PMID: 26752241
- PMCID: PMC4707491
- DOI: 10.1038/srep19093
Pharmacologic Interventions in Preventing Ovarian Hyperstimulation Syndrome: A Systematic Review and Network Meta-Analysis
Abstract
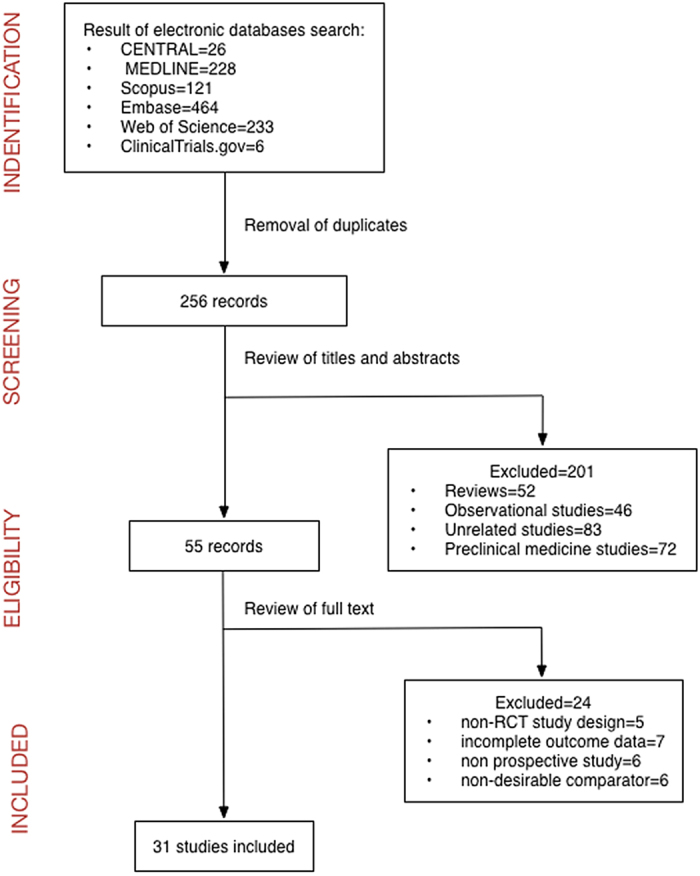
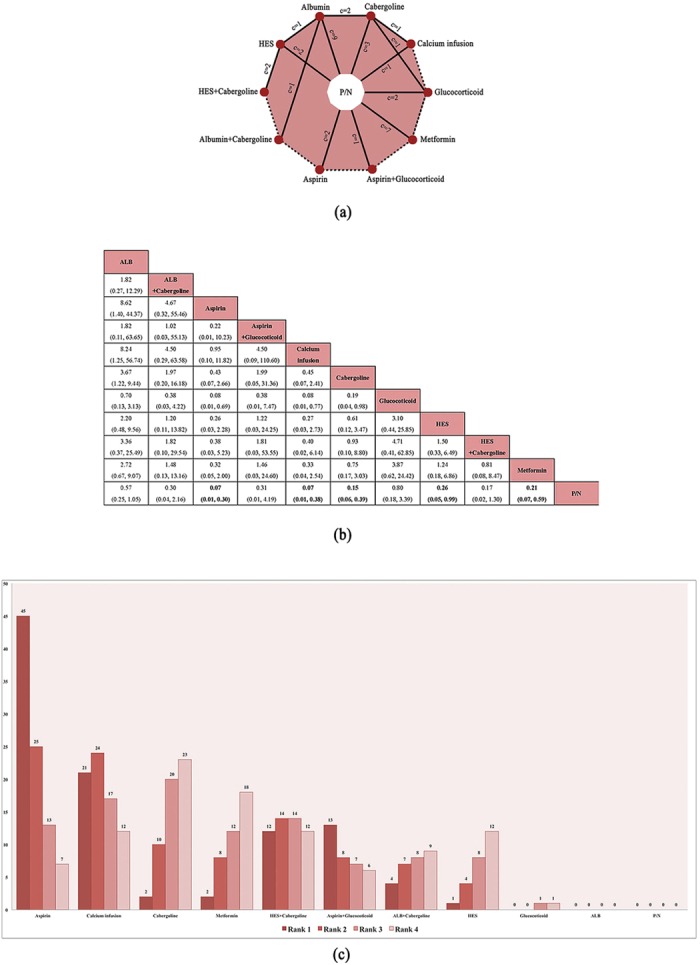
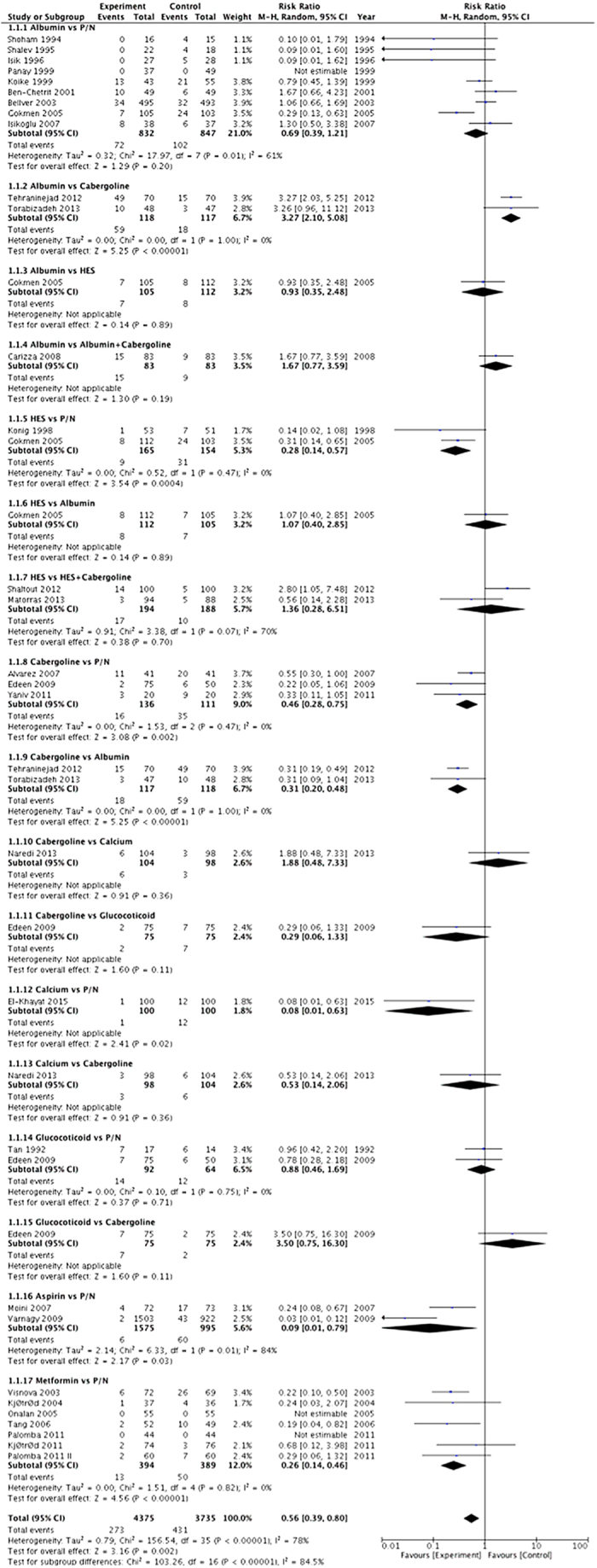
Ovarian hyperstimulation syndrome (OHSS) is a severe iatrogenic complication of controlled ovarian stimulation. Randomised controlled trials (RCTs) have proven several pharmacologic interventions to be effective in OHSS prevention, but these trials have seldom compared multiple drugs. We identified randomised controlled trials (RCTs) through June 2015 by searching databases and compared 11 intervention strategies in preventing OHSS (primary outcome) and their influence on pregnancy rate (secondary outcome). A network meta-analysis was used to evaluate the relative effectiveness among treatments and to create a rank probability table. Thirty-one RCTs were identified, including 7181 participants. Five pharmacologic interventions were superior to placebo in decreasing OHSS incidence: aspirin [relative risk (RR) 0.07, 95% credible interval (CrI) 0.01-0.30, p < 0.05], intravenous (IV) calcium [RR 0.11, 95% CrI 0.02-0.54, p < 0.05], cabergoline [RR 0.17, 95% CrI 0.06-0.43, p < 0.05], metformin [RR 0.20, 95% CrI 0.07-0.59, p < 0.05] and IV hydroxyethyl starch (HES) [RR 0.26, 95% CrI 0.05-0.99, p < 0.05]. The rank probability demonstrated aspirin (Rank 1: 36%) and IV calcium (Rank 1: 35%) to be the most efficacious. Additionally, albumin might decrease the pregnancy rate when compared with placebo [RR 0.85, 95% CI 0.74-0.97, p < 0.05]. This conclusion provides a relative standard and objective reference for choosing an OHSS prophylactic agent.
Figures
References
-
- Garcia-Velasco J. A. & Pellicer A. New concepts in the understanding of the ovarian hyperstimulation syndrome. Curr Opin Obstet Gynecol 15, 251–6 (2003). - PubMed
-
- Binder H. et al. Update on ovarian hyperstimulation syndrome: Part 1–Incidence and pathogenesis. Int J Fertil Womens Med 52, 11–26 (2007). - PubMed
-
- Delvigne A. & Rozenberg S. A qualitative systematic review of coasting, a procedure to avoid ovarian hyperstimulation syndrome in IVF patients. Hum Reprod Update 8, 291–6 (2002). - PubMed
-
- Emperaire J. C. & Ruffie A. Triggering ovulation with endogenous luteinizing hormone may prevent the ovarian hyperstimulation syndrome. Hum Reprod 6, 506–10 (1991). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
