

Proton Pump Inhibitor Use and the Risk of Chronic Kidney Disease
- PMID: 26752337
- PMCID: PMC4772730
- DOI: 10.1001/jamainternmed.2015.7193
Proton Pump Inhibitor Use and the Risk of Chronic Kidney Disease
Abstract
Importance: Proton pump inhibitors (PPIs) are among the most commonly used drugs worldwide and have been linked to acute interstitial nephritis. Less is known about the association between PPI use and chronic kidney disease (CKD).
Objective: To quantify the association between PPI use and incident CKD in a population-based cohort.
Design, setting, and participants: In total, 10,482 participants in the Atherosclerosis Risk in Communities study with an estimated glomerular filtration rate of at least 60 mL/min/1.73 m(2) were followed from a baseline visit between February 1, 1996, and January 30, 1999, to December 31, 2011. The data was analyzed from May 2015 to October 2015. The findings were replicated in an administrative cohort of 248,751 patients with an estimated glomerular filtration rate of at least 60 mL/min/1.73 m(2) from the Geisinger Health System.
Exposures: Self-reported PPI use in the Atherosclerosis Risk in Communities study or an outpatient PPI prescription in the Geisinger Health System replication cohort. Histamine2 (H2) receptor antagonist use was considered a negative control and active comparator.
Main outcomes and measures: Incident CKD was defined using diagnostic codes at hospital discharge or death in the Atherosclerosis Risk in Communities Study, and by a sustained outpatient estimated glomerular filtration rate of less than 60 mL/min/1.73 m(2) in the Geisinger Health System replication cohort.
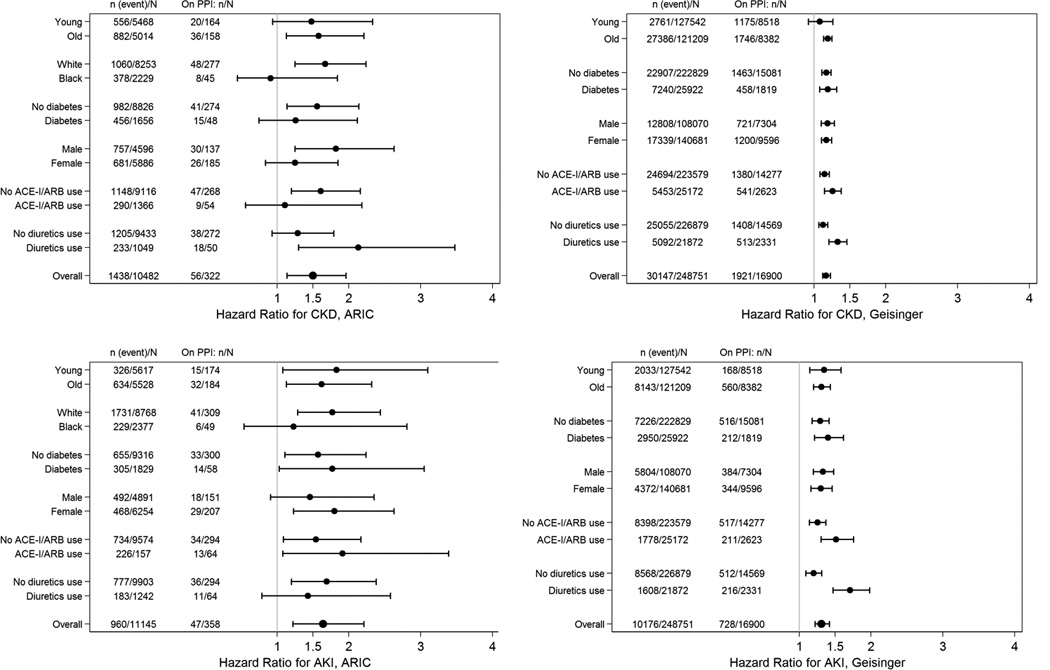
Results: Among 10,482 participants in the Atherosclerosis Risk in Communities study, the mean (SD) age was 63.0 (5.6) years, and 43.9% were male. Compared with nonusers, PPI users were more often of white race, obese, and taking antihypertensive medication. Proton pump inhibitor use was associated with incident CKD in unadjusted analysis (hazard ratio [HR], 1.45; 95% CI, 1.11-1.90); in analysis adjusted for demographic, socioeconomic, and clinical variables (HR, 1.50; 95% CI, 1.14-1.96); and in analysis with PPI ever use modeled as a time-varying variable (adjusted HR, 1.35; 95% CI, 1.17-1.55). The association persisted when baseline PPI users were compared directly with H2 receptor antagonist users (adjusted HR, 1.39; 95% CI, 1.01-1.91) and with propensity score-matched nonusers (HR, 1.76; 95% CI, 1.13-2.74). In the Geisinger Health System replication cohort, PPI use was associated with CKD in all analyses, including a time-varying new-user design (adjusted HR, 1.24; 95% CI, 1.20-1.28). Twice-daily PPI dosing (adjusted HR, 1.46; 95% CI, 1.28-1.67) was associated with a higher risk than once-daily dosing (adjusted HR, 1.15; 95% CI, 1.09-1.21).
Conclusions and relevance: Proton pump inhibitor use is associated with a higher risk of incident CKD. Future research should evaluate whether limiting PPI use reduces the incidence of CKD.
Figures
Comment in
- Dtsch Med Wochenschr. 2016 Apr;141(8):532
-
Adverse Effects Associated With Proton Pump Inhibitors.JAMA Intern Med. 2016 Feb;176(2):172-4. doi: 10.1001/jamainternmed.2015.7927. JAMA Intern Med. 2016. PMID: 26751904 No abstract available.
-
Proton pump inhibitors are associated with risk of chronic kidney disease, study finds.BMJ. 2016 Jan 12;352:i128. doi: 10.1136/bmj.i128. BMJ. 2016. PMID: 26759185 No abstract available.
-
Therapy: Risks associated with chronic PPI use - signal or noise?Nat Rev Gastroenterol Hepatol. 2016 May;13(5):253-4. doi: 10.1038/nrgastro.2016.44. Epub 2016 Mar 16. Nat Rev Gastroenterol Hepatol. 2016. PMID: 27006255 No abstract available.
-
PPI können die Nieren schädigen.Praxis (Bern 1994). 2016 Apr 13;105(8):471-2. doi: 10.1024/1661-8157/a002326. Praxis (Bern 1994). 2016. PMID: 27078733 German. No abstract available.
-
Adverse Effects of Proton Pump Inhibitors in Chronic Kidney Disease.JAMA Intern Med. 2016 Jun 1;176(6):866. doi: 10.1001/jamainternmed.2016.1845. JAMA Intern Med. 2016. PMID: 27273493 No abstract available.
-
Adverse Effects of Proton Pump Inhibitors in Chronic Kidney Disease.JAMA Intern Med. 2016 Jun 1;176(6):866-7. doi: 10.1001/jamainternmed.2016.1848. JAMA Intern Med. 2016. PMID: 27273494 No abstract available.
-
Adverse Effects of Proton Pump Inhibitors in Chronic Kidney Disease.JAMA Intern Med. 2016 Jun 1;176(6):867. doi: 10.1001/jamainternmed.2016.1851. JAMA Intern Med. 2016. PMID: 27273495 No abstract available.
-
Adverse Effects of Proton Pump Inhibitors in Chronic Kidney Disease.JAMA Intern Med. 2016 Jun 1;176(6):867-8. doi: 10.1001/jamainternmed.2016.1854. JAMA Intern Med. 2016. PMID: 27273496 No abstract available.
-
Adverse Effects of Proton Pump Inhibitors in Chronic Kidney Disease.JAMA Intern Med. 2016 Jun 1;176(6):868. doi: 10.1001/jamainternmed.2016.1857. JAMA Intern Med. 2016. PMID: 27273497 No abstract available.
-
Adverse Effects of Proton Pump Inhibitors in Chronic Kidney Disease.JAMA Intern Med. 2016 Jun 1;176(6):868-9. doi: 10.1001/jamainternmed.2016.1860. JAMA Intern Med. 2016. PMID: 27273498 No abstract available.
-
Adverse Effects of Proton Pump Inhibitors in Chronic Kidney Disease-Reply.JAMA Intern Med. 2016 Jun 1;176(6):869-70. doi: 10.1001/jamainternmed.2016.1863. JAMA Intern Med. 2016. PMID: 27273499 No abstract available.
References
-
- United States Renal Data System. 2014 USRDS Annual Data Report: An overview of the epidemiology of kidney disease in the United States. 2014.
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004 Sep 23;351(13):1296–1305. - PubMed
-
- Coresh J, Selvin E, Stevens LA, et al. Prevalence of chronic kidney disease in the United States. JAMA. 2007 Nov 7;298(17):2038–2047. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/PHS HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- K23 DK106515/DK/NIDDK NIH HHS/United States
- HHSN268201100009C/PHS HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- K08DK092287/DK/NIDDK NIH HHS/United States
- HHSN268201100010C/PHS HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/PHS HHS/United States
- HHSN268201100012C/PHS HHS/United States
- K23 DK097201/DK/NIDDK NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- HHSN268201100007C/PHS HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/PHS HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
- K08 DK092287/DK/NIDDK NIH HHS/United States
- HHSN268201100006C/PHS HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
