

Does malalignment affect revision rate in total knee replacements: a systematic review of the literature
- PMID: 26753122
- PMCID: PMC4695472
- DOI: 10.1186/s40064-015-1604-4
Does malalignment affect revision rate in total knee replacements: a systematic review of the literature
Abstract
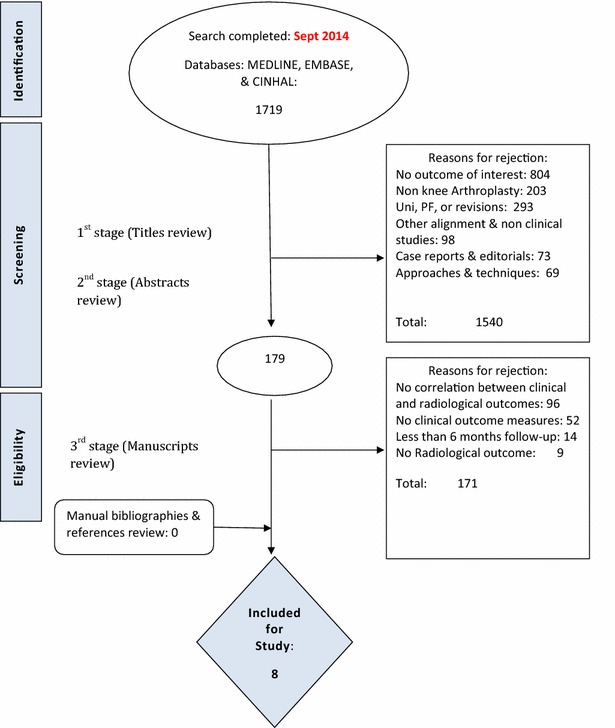
To ensure implant durability following Modern total knee replacement (TKR) surgery, one long held principle in condylar total knee arthroplasty is positioning the components in alignment with the mechanical axis and restoring the overall limb alignment to 180° ± 3°. However, this view has been challenged recently. Given the high number of TKR performed, clarity on this integral aspect of the procedure is necessary. To investigate the association between malalignment following primary TKR and revision rates. A systematic review of the literature was conducted using a computerised literature search of Medline, CINHAL, and EMBASE to identify English-language studies published from 2000 through to 2014. Studies with adequate information on the correlation between malalignment and revision rate with a minimum follow-up of 6 months were considered for inclusion. A study protocol, including the detailed search strategy was published on the PROSPERO database for systematic reviews. From an initial 2107 citations, eight studies, with variable methodological qualities, were eligible for inclusion. Collectively, nine parameters of alignment were studied, and 20 assessments were made between an alignment parameter and revision rate. Four out of eight studies demonstrated an association between a malalignment parameter and increased revision rates. In the coronal plane, only three studies assessed the mechanical axis. None of these studies found an association with revision rates, whereas four of the five studies investigating the anatomical axis found an association between malalignment and increased revision rate. This study demonstrates the effect of malalignment on revision rates is likely to be modest. Interestingly, studies that used mechanical alignment in the coronal plane demonstrated no association with revision rates. This questions the premise of patient specific instrumentation devices based on the mechanically aligned knee when considering revision as the endpoint.
Keywords: Malalignment; Revision rate; Systematic review; Total knee arthroplasty.
Figures
References
-
- Bargren JH, Blaha JD, Freeman MA. Alignment in total knee arthroplasty. Correlated biomechanical and clinical observations. Clin Orthop Relat Res. 1983;173:178–183. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
