

Mechanical Thrombectomy in Stroke
- PMID: 26754120
- PMCID: PMC4711295
- DOI: 10.3238/arztebl.2015.0830
Mechanical Thrombectomy in Stroke
Abstract
Background: The introduction of neurological stroke units and of thrombolysis with the intravenous (IV) administration of recombinant tissue-type plasminogen activator (tPA) have markedly improved the treatment of stroke. Five randomized trials of catheter-based interventional treatment of stroke with special stents were published in 2015.
Methods: Recently published randomized trials of mechanical thrombectomy are selectively reviewed.
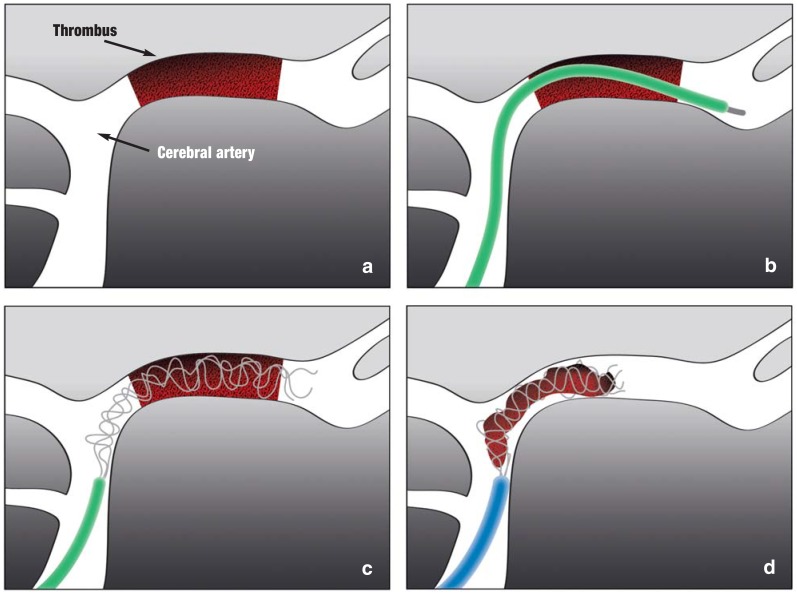
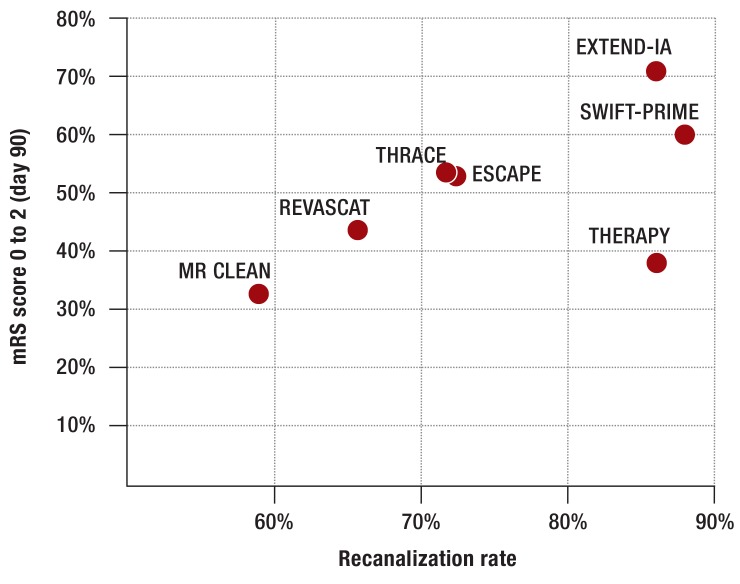
Results: These trials documented the clinical efficacy of mechanical thrombectomy (MT) in the treatment of occlusion of a major cerebral artery in the distribution of the internal carotid artery (evidence level 1a, recommendation grade A). Roughly 4-10% of all stroke patients could benefit from such an intervention. In the trials, 85% of the patients were first treated with IV-tPA. A recanalization of the occluded vessel was achieved by MT in 59-88% of patients. The percentage of patients with no deficit or only a mild deficit was 33-71% among those who received the intervention, compared to 19-40% in the control groups. The trial data indicate that MT is effective for elderly patients as well (age over 80). Thrombectomy did not increase the rate of secondary, symptomatic intracranial hemorrhage.
Conclusion: MT can only be used to treat the occlusion of major cerebral arteries. In appropriate patients, it expands the spectrum of treatment options for stroke. Long-term data are not yet available.
Figures
Comment in
-
Intra-arterial Treatment.Dtsch Arztebl Int. 2016 May 27;113(21):375. doi: 10.3238/arztebl.2016.0375a. Dtsch Arztebl Int. 2016. PMID: 27504704 Free PMC article. No abstract available.
References
-
- Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med. 1995;333:1581–1587. - PubMed
-
- Langhorne P, Williams BO, Gilchrist W, Howie K. Do stroke units save lives? Lancet. 1993;342:395–398. - PubMed
-
- Bogousslavsky J, van Melle G, Regli F. The Lausanne Stroke Registry: analysis of 1,000 consecutive patients with first stroke. Stroke. 1988;19:1083–1092. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical