

Plasma Biomarkers Reflecting Profibrotic Processes in Heart Failure With a Preserved Ejection Fraction: Data From the Prospective Comparison of ARNI With ARB on Management of Heart Failure With Preserved Ejection Fraction Study
- PMID: 26754625
- PMCID: PMC5485256
- DOI: 10.1161/CIRCHEARTFAILURE.115.002551
Plasma Biomarkers Reflecting Profibrotic Processes in Heart Failure With a Preserved Ejection Fraction: Data From the Prospective Comparison of ARNI With ARB on Management of Heart Failure With Preserved Ejection Fraction Study
Abstract
Background: Heart failure with preserved ejection fraction is a clinical syndrome that has been associated with changes in the extracellular matrix. The purpose of this study was to determine whether profibrotic biomarkers accurately reflect the presence and severity of disease and underlying pathophysiology and modify response to therapy in patients with heart failure with preserved ejection fraction.
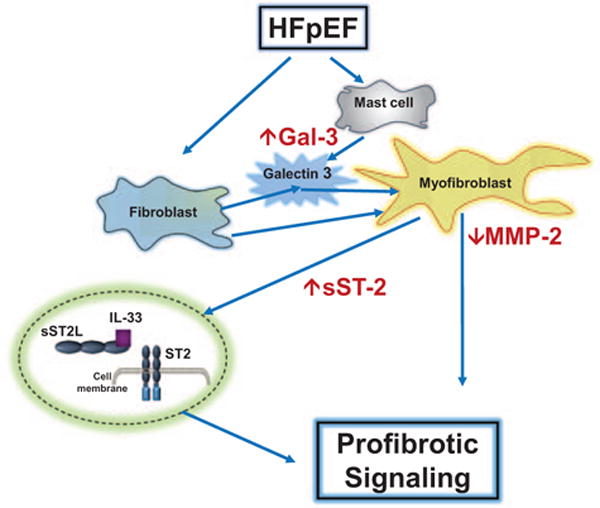
Methods and results: Four biomarkers, soluble form of ST2 (an interleukin-1 receptor family member), galectin-3, matrix metalloproteinase-2, and collagen III N-terminal propeptide were measured in the Prospective Comparison of ARNI With ARB on Management of Heart Failure With Preserved Ejection Fraction (PARAMOUNT) trial at baseline, 12 and 36 weeks after randomization to valsartan or LCZ696. We examined the relationship between baseline biomarkers, demographic and echocardiographic characteristics, change in primary (change in N-terminal pro B-type natriuretic peptide) and secondary (change in left atrial volume) end points. The median (interquartile range) value for soluble form of ST2 (33 [24.6-48.1] ng/mL) and galectin 3 (17.8 [14.1-22.8] ng/mL) were higher, and for matrix metalloproteinase-2 (188 [155.5-230.6] ng/mL) lower, than in previously published referent controls; collagen III N-terminal propeptide (5.6 [4.3-6.9] ng/mL) was similar to referent control values. All 4 biomarkers correlated with severity of disease as indicated by N-terminal pro B-type natriuretic peptide, E/E', and left atrial volume. Baseline biomarkers did not modify the response to LCZ696 for lowering N-terminal pro B-type natriuretic peptide; however, left atrial volume reduction varied by baseline level of soluble form of ST2 and galectin 3; patients with values less than the observed median (<33 ng/mL soluble form of ST2 and <17.8 ng/mL galectin 3) had reduction in left atrial volume, those above median did not. Although LCZ696 reduced N-terminal pro B-type natriuretic peptide, levels of the other 4 biomarkers were not affected over time.
Conclusions: In patients with heart failure with preserved ejection fraction, biomarkers that reflect collagen homeostasis correlated with the presence and severity of disease and underlying pathophysiology, and may modify the structural response to treatment.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT00887588.
Keywords: biomarkers; extracellular matrix; heart failure; homeostasis; pathophysiology.
© 2016 American Heart Association, Inc.
Conflict of interest statement
Drs Zile, Solomon, Pieske, Voors, and McMurray have received research support and have consulted for Novartis. Dr Jhund has consulted for Novartis. Drs Shi, Prescott, and Lefkowitz are employees of Novartis. The other authors report no conflicts.
Figures


References
-
- Ahmad T, Fiuzat M, Pencina MJ, Geller NL, Zannad F, Cleland JG, Snider JV, Blankenberg S, Adams KF, Redberg RF, Kim JB, Mascette A, Mentz RJ, O’Connor CM, Felker GM, Januzzi IL. Charting a roadmap for heart failure biomarker studies. JACC Heart Fail. 2014;2:477–488. doi: 10.1016/j.jchf.2014.02.005. - DOI - PMC - PubMed
-
- Zile MR, Desantis SM, Baicu CF, Stroud RE, Thompson SB, McClure CD, Mehurg SM, Spinale FG. Plasma biomarkers that reflect determinants of matrix composition identify the presence of left ventricular hypertrophy and diastolic heart failure. Circ Heart Fail. 2011;4:246–256. doi: 10.1161/CIRCHEARTFAILURE.110.958199. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
