

Wide field of view swept-source optical coherence tomography for peripheral retinal disease
- PMID: 26755643
- PMCID: PMC5088499
- DOI: 10.1136/bjophthalmol-2015-307480
Wide field of view swept-source optical coherence tomography for peripheral retinal disease
Abstract
Background/aims: To assess peripheral retinal lesions and the posterior pole in single widefield optical coherence tomography (OCT) volumes.
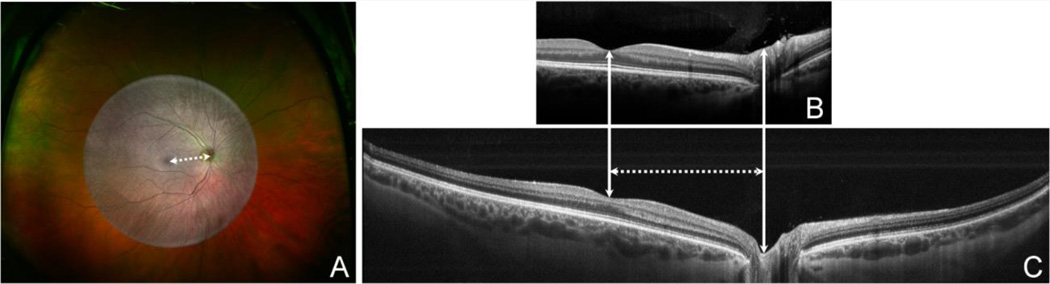
Methods: A wide field of view (FOV) swept-source OCT (WFOV SSOCT) system was developed using a commercial swept-source laser and a custom sample arm consisting of two indirect ophthalmic lenses. Twenty-seven subjects with peripheral lesions (choroidal melanomas, choroidal naevi, sclerochoroidal calcification, retinitis pigmentosa, diabetic retinopathy, retinoschisis and uveitis) were imaged with the WFOV SSOCT. Volumes were taken in primary gaze. Using the optic nerve to fovea distance as a reference measurement, comparisons were made between the lateral FOV of the WFOV SSOCT, current generation spectral-domain OCT (SDOCT) and widefield scanning laser ophthalmoscopy (SLO) of the same eyes.
Results: Peripheral pathologies were captured with WFOV SSOCT in 26 of the 27 subjects. The one not captured was in the far nasal periphery and was not seen in the primary gaze volume. Posterior pole associated pathologies were captured in all subjects. Current generation SDOCT had a mean lateral FOV of 2.08±0.21 optic nerve to fovea distance units, WFOV SSOCT had an FOV of 4.62±0.62 units and SLO had an FOV of 9.35±1.02 units.
Conclusions: WFOV OCT can be used to examine both peripheral retinal pathology and the posterior pole within a single volume acquisition. SLO had the greatest FOV, but does not provide depth information. Future studies using widefield OCT systems will help further delineate the role of WFOV OCT to quantitatively assess and monitor peripheral retinal disease in three dimensions.
Keywords: Imaging; Retina.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures




References
-
- Swanson EA. OCT technology transfer and the OCT market. In: Drexler W, Fujimoto JG, editors. Optical coherence tomography. New York: Springer; 2015. pp. 2529–2571.
-
- Schuman JS, Puliafito CA, Fujimoto JG, Duker JS. Optical coherence tomography of ocular disease. 3rd. Thorofare, NJ: SLACK incorporated; 2012. pp. 3–26.
-
- Shields CL, Materin MA, Shields JA. Review of optical coherence tomography for intraocular tumors. Curr Opin Ophthalmol. 2005 Jun;16(3):141–154. - PubMed
-
- Torres VL, Brugnoni N, Kaiser PK, et al. Optical coherence tomography enhanced depth imaging of choroidal tumors. Am J Ophthalmol. 2011 Apr;151(4):586–593. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical