

Distinctive aspects of peptic ulcer disease, Dieulafoy's lesion, and Mallory-Weiss syndrome in patients with advanced alcoholic liver disease or cirrhosis
- PMID: 26755890
- PMCID: PMC4698507
- DOI: 10.3748/wjg.v22.i1.446
Distinctive aspects of peptic ulcer disease, Dieulafoy's lesion, and Mallory-Weiss syndrome in patients with advanced alcoholic liver disease or cirrhosis
Abstract
Aim: To systematically review the data on distinctive aspects of peptic ulcer disease (PUD), Dieulafoy's lesion (DL), and Mallory-Weiss syndrome (MWS) in patients with advanced alcoholic liver disease (aALD), including alcoholic hepatitis or alcoholic cirrhosis.
Methods: Computerized literature search performed via PubMed using the following medical subject heading terms and keywords: "alcoholic liver disease", "alcoholic hepatitis"," alcoholic cirrhosis", "cirrhosis", "liver disease", "upper gastrointestinal bleeding", "non-variceal upper gastrointestinal bleeding", "PUD", ''DL'', ''Mallory-Weiss tear", and "MWS''.
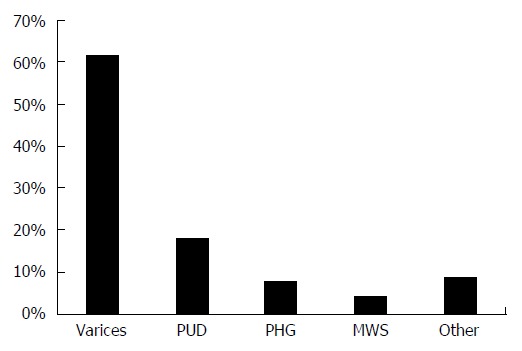
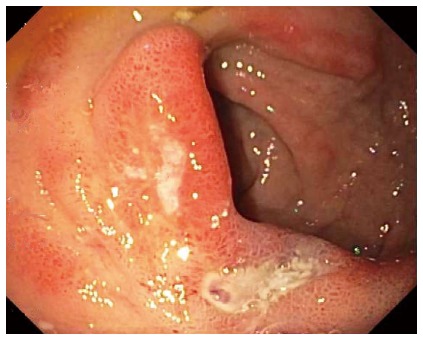
Results: While the majority of acute gastrointestinal (GI) bleeding with aALD is related to portal hypertension, about 30%-40% of acute GI bleeding in patients with aALD is unrelated to portal hypertension. Such bleeding constitutes an important complication of aALD because of its frequency, severity, and associated mortality. Patients with cirrhosis have a markedly increased risk of PUD, which further increases with the progression of cirrhosis. Patients with cirrhosis or aALD and peptic ulcer bleeding (PUB) have worse clinical outcomes than other patients with PUB, including uncontrolled bleeding, rebleeding, and mortality. Alcohol consumption, nonsteroidal anti-inflammatory drug use, and portal hypertension may have a pathogenic role in the development of PUD in patients with aALD. Limited data suggest that Helicobacter pylori does not play a significant role in the pathogenesis of PUD in most cirrhotic patients. The frequency of bleeding from DL appears to be increased in patients with aALD. DL may be associated with an especially high mortality in these patients. MWS is strongly associated with heavy alcohol consumption from binge drinking or chronic alcoholism, and is associated with aALD. Patients with aALD have more severe MWS bleeding and are more likely to rebleed when compared to non-cirrhotics. Pre-endoscopic management of acute GI bleeding in patients with aALD unrelated to portal hypertension is similar to the management of aALD patients with GI bleeding from portal hypertension, because clinical distinction before endoscopy is difficult. Most patients require intensive care unit admission and attention to avoid over-transfusion, to correct electrolyte abnormalities and coagulopathies, and to administer antibiotic prophylaxis. Alcoholics should receive thiamine and be closely monitored for symptoms of alcohol withdrawal. Prompt endoscopy, after initial resuscitation, is essential to diagnose and appropriately treat these patients. Generally, the same endoscopic hemostatic techniques are used in patients bleeding from PUD, DL, or MWS in patients with aALD as in the general population.
Conclusion: Nonvariceal upper GI bleeding in patients with aALD has clinically important differences from that in the general population without aALD, including: more frequent and more severe bleeding from PUD, DL, or MWS.
Keywords: Alcoholic hepatitis; Alcoholic liver disease; Cirrhosis; Dieulafoy lesion; Endoscopic therapy; Mallory-Weiss syndrome; Peptic ulcer disease; Portal hypertension.
Figures
Similar articles
-
Non-variceal gastrointestinal bleeding in patients with liver cirrhosis: a review.Dig Dis Sci. 2012 Nov;57(11):2743-54. doi: 10.1007/s10620-012-2229-x. Epub 2012 Jun 4. Dig Dis Sci. 2012. PMID: 22661272 Review.
-
Endoscopic hemostasis of nonvariceal, non-peptic ulcer hemorrhage.Gastrointest Endosc Clin N Am. 1997 Oct;7(4):657-70. Gastrointest Endosc Clin N Am. 1997. PMID: 9376956 Review.
-
Frequency, significance and therapy of the Mallory-Weiss syndrome in patients with portal hypertension.Hepatology. 1990 May;11(5):879-83. doi: 10.1002/hep.1840110525. Hepatology. 1990. PMID: 2347558
-
Diagnosis and management of nonvariceal upper gastrointestinal hemorrhage: European Society of Gastrointestinal Endoscopy (ESGE) Guideline.Endoscopy. 2015 Oct;47(10):a1-46. doi: 10.1055/s-0034-1393172. Epub 2015 Sep 29. Endoscopy. 2015. PMID: 26417980
-
A prospective endoscopic evaluation of the causes of upper GI hemorrhage in alcoholics: a focus on alcoholic gastropathy.Am J Gastroenterol. 1996 Jul;91(7):1343-7. Am J Gastroenterol. 1996. PMID: 8677991
Cited by
-
Peptic ulcer disease in non-alcoholic fatty liver disease hospitalizations: A new challenge on the horizon in the United States.World J Hepatol. 2023 Apr 27;15(4):564-576. doi: 10.4254/wjh.v15.i4.564. World J Hepatol. 2023. PMID: 37206652 Free PMC article.
-
Somatic comorbidities of inpatients receiving treatment for alcohol withdrawal syndrome on a psychiatric ward and their relation to delirium tremens.Postep Psychiatr Neurol. 2021 Dec;30(4):219-230. doi: 10.5114/ppn.2021.111918. Epub 2021 Dec 21. Postep Psychiatr Neurol. 2021. PMID: 37082559 Free PMC article.
-
Inpatient outcomes of Dieulafoy's lesions in the United States.Proc (Bayl Univ Med Cent). 2022 Mar 15;35(3):291-296. doi: 10.1080/08998280.2022.2043806. eCollection 2022. Proc (Bayl Univ Med Cent). 2022. PMID: 35518828 Free PMC article.
-
Recurrence of Multiple Gastrointestinal Angioectasias Despite Treatment with Argon Plasma Coagulation Requiring Thalidomide Treatment in a Patient with Cirrhosis: A Rare Case Report.Cureus. 2019 Mar 6;11(3):e4196. doi: 10.7759/cureus.4196. Cureus. 2019. PMID: 31106096 Free PMC article.
-
Immunotherapy in hepatocellular carcinoma: evaluation and management of adverse events associated with atezolizumab plus bevacizumab.Ther Adv Med Oncol. 2021 Jul 29;13:17588359211031141. doi: 10.1177/17588359211031141. eCollection 2021. Ther Adv Med Oncol. 2021. PMID: 34377156 Free PMC article. Review.
References
-
- World Health Organization. Global status report on alcohol and health. Geneva: World Health Organization; 2011. p. 286.
-
- Welte J, Barnes G, Wieczorek W, Tidwell MC, Parker J. Alcohol and gambling pathology among U.S. adults: prevalence, demographic patterns and comorbidity. J Stud Alcohol. 2001;62:706–712. - PubMed
-
- Rehm J, Samokhvalov AV, Shield KD. Global burden of alcoholic liver diseases. J Hepatol. 2013;59:160–168. - PubMed
-
- Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murray CJ. Selected major risk factors and global and regional burden of disease. Lancet. 2002;360:1347–1360. - PubMed
-
- MacSween RN, Burt AD. Histologic spectrum of alcoholic liver disease. Semin Liver Dis. 1986;6:221–232. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
