

Acute and Chronic Kidney Disease and Cardiovascular Mortality After Major Surgery
- PMID: 26756753
- PMCID: PMC4936961
- DOI: 10.1097/SLA.0000000000001582
Acute and Chronic Kidney Disease and Cardiovascular Mortality After Major Surgery
Abstract
Objective: The aim of the study was to determine the long-term cardiovascular-specific mortality in patients with acute kidney injury (AKI) or chronic kidney disease (CKD) after major surgery.
Background: In surgical patients, pre-existing CKD and postoperative AKI are associated with increases in all-cause mortality.
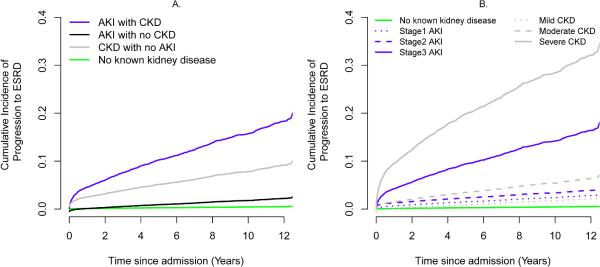
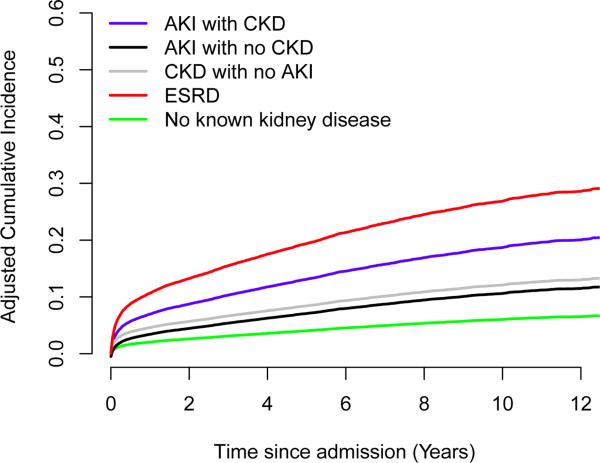
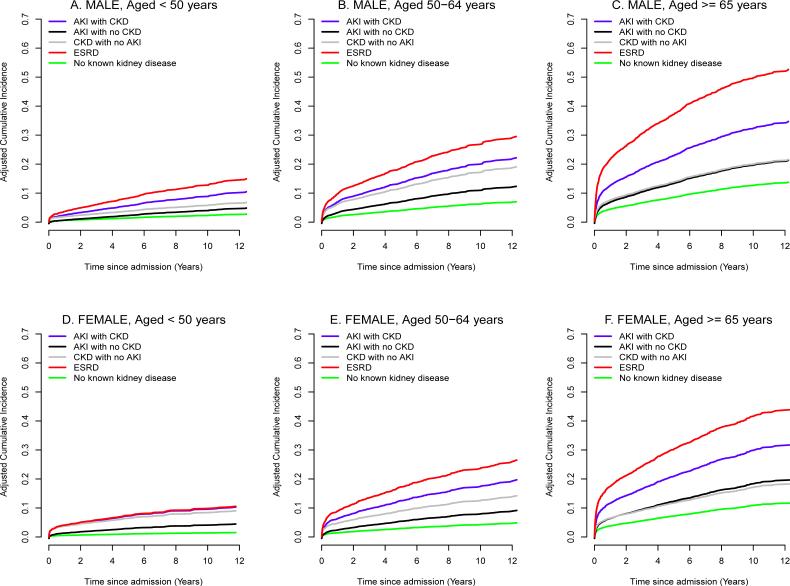
Methods: In a single-center cohort of 51,457 adult surgical patients undergoing major inpatient surgery, long-term cardiovascular-specific mortality was modeled using a multivariable subdistributional hazards model while treating any other cause of death as a competing risk and accounting for the progression to end-stage renal disease (ESRD) after discharge. Pre-existing CKD and ESRD, and postoperative AKI were the main independent predictors.
Results: Before the admission, 4% and 8% of the cohort had pre-existing ESRD and CKD not requiring renal replacement therapy, respectively. During hospitalization, 39% developed AKI. At 10-year follow-up, adjusted cardiovascular-specific mortality estimates were 6%, 11%, 12%, 19%, and 27% for patients with no kidney disease, AKI with no CKD, CKD with no AKI, AKI with CKD, and ESRD, respectively (P < 0.001). This association remained after excluding 916 patients who progressed to ESRD after discharge, although it was significantly amplified among them. Compared with patients having no kidney disease, adjusted hazard ratios for cardiovascular mortality were significantly higher among patients with kidney disease, ranging from 1.95 (95% confidence interval, 1.80-2.11) for patients with de novo AKI to 5.70 (95% confidence interval, 5.00-6.49) for patients with pre-existing ESRD.
Conclusions: Both AKI and CKD were associated with higher long-term cardiovascular-specific mortality compared with patients having no kidney disease.
Figures
References
-
- Bihorac A, Yavas S, Subbiah S, et al. Long-term risk of mortality and acute kidney injury during hospitalization after major surgery. Ann Surg. 2009;249:851–858. - PubMed
-
- Hobson CE, Yavas S, Segal MS, et al. Acute kidney injury is associated with increased long-term mortality after cardiothoracic surgery. Circulation. 2009;119:2444–2453. - PubMed
-
- Wald R, Quinn RR, Luo J. Chronic dialysis and death among survivors of acute kidney injury requiring dialysis. JAMA. 2009;302:1179–1185. - PubMed
-
- Ishani A, Nelson D, Clothier B, et al. The magnitude of acute serum creatinine increase after cardiac surgery and the risk of chronic kidney disease, progression of kidney disease, and death. Arch Intern Med. 2011;171:226–233. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
