

Fentanyl and Midazolam Are Ineffective in Reducing Episodic Intracranial Hypertension in Severe Pediatric Traumatic Brain Injury
- PMID: 26757162
- PMCID: PMC5005007
- DOI: 10.1097/CCM.0000000000001558
Fentanyl and Midazolam Are Ineffective in Reducing Episodic Intracranial Hypertension in Severe Pediatric Traumatic Brain Injury
Abstract
Objective: To evaluate the clinical effectiveness of bolus-dose fentanyl and midazolam to treat episodic intracranial hypertension in children with severe traumatic brain injury.
Design: Retrospective cohort.
Setting: PICU in a university-affiliated children's hospital level I trauma center.
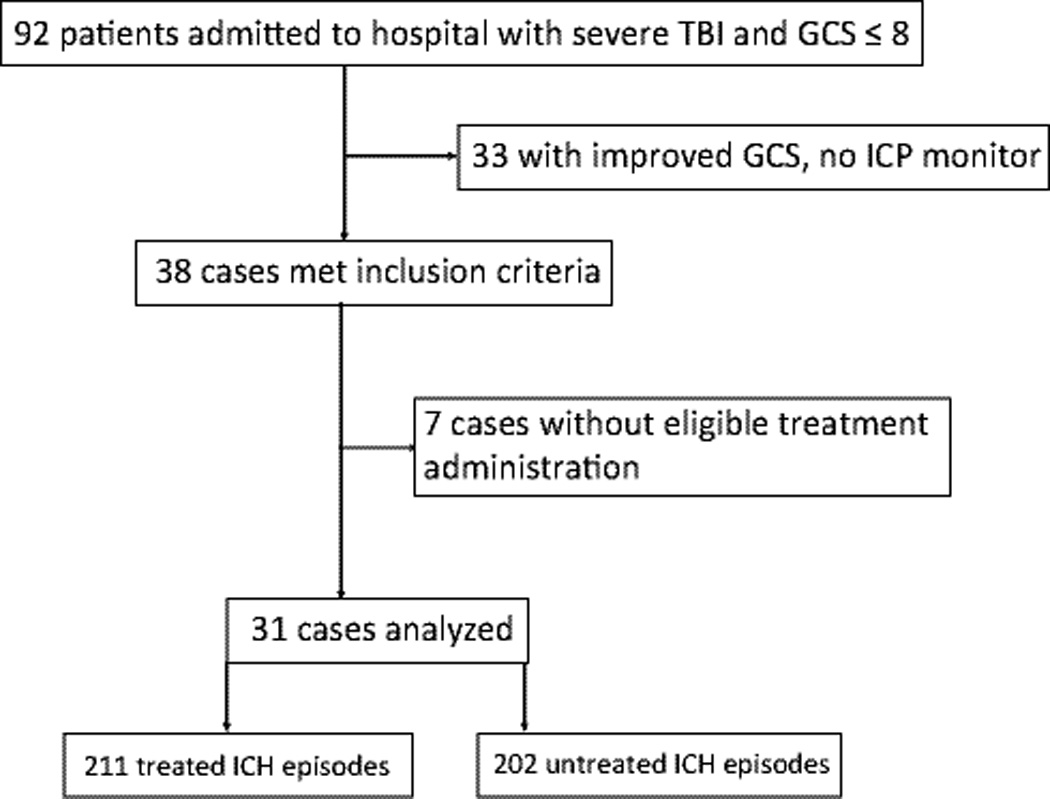
Patients: Thirty-one children 0-18 years of age with severe traumatic brain injury (Glasgow Coma Scale score of ≤ 8) who received bolus doses of fentanyl and/or midazolam for treatment of episodic intracranial hypertension.
Interventions: None.
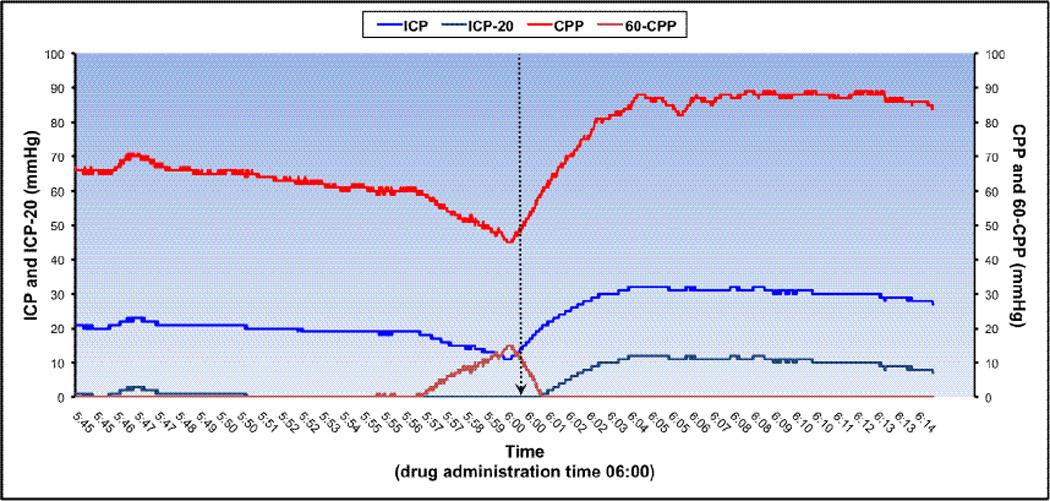
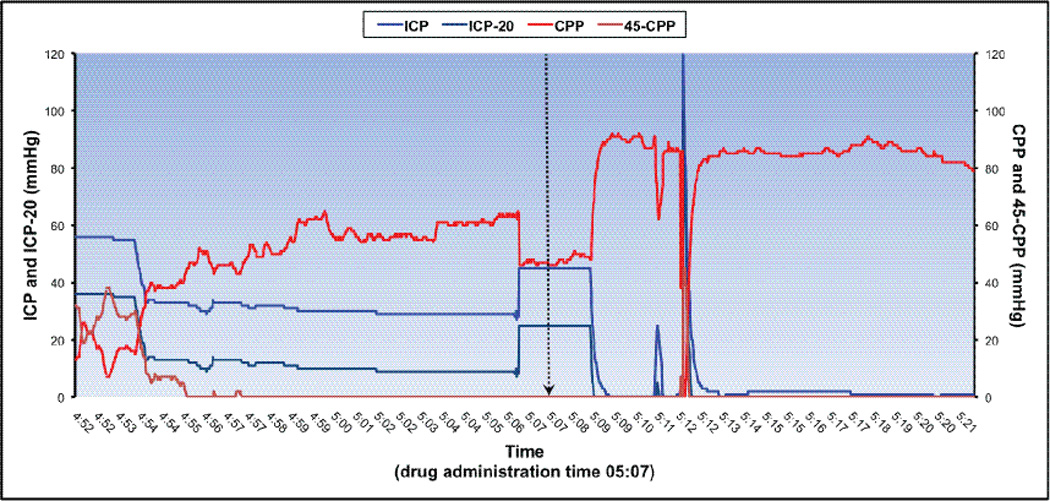
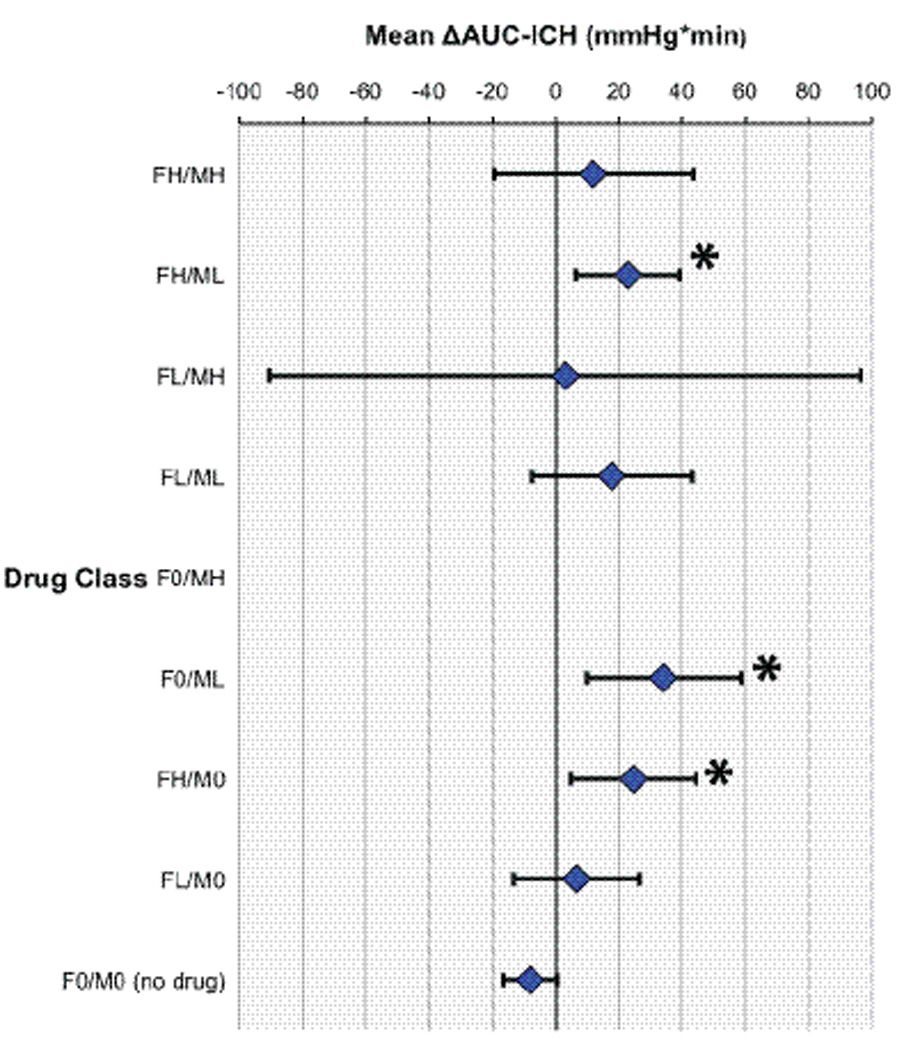
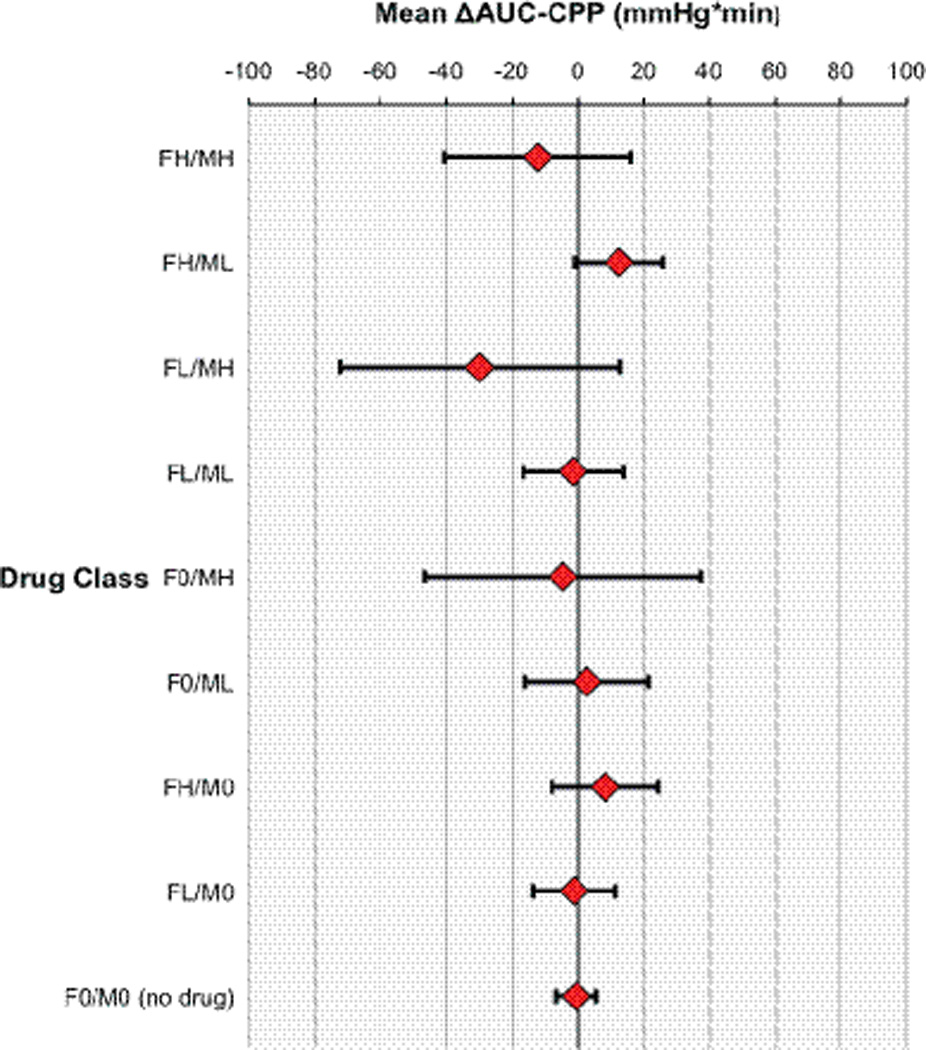
Measurements and main results: The area under the curve from high-resolution intracranial pressure-time plots was calculated to represent cumulative intracranial hypertension exposure: area under the curve for intracranial pressure above 20 mm Hg (area under the curve-intracranial hypertension) was calculated in 15-minute epochs before and after administration of fentanyl and/or midazolam for the treatment of episodic intracranial hypertension. Our primary outcome measure, the difference between predrug and postdrug administration epochs (Δarea under the curve-intracranial hypertension), was calculated for all occurrences. We examined potential covariates including age, injury severity, mechanism, and time after injury; time after injury correlated with Δarea under the curve-intracranial hypertension. In a mixed-effects model, with patient as a random effect, drug/dose combination as a fixed effect, and time after injury as a covariate, intracranial hypertension increased after administration of fentanyl and/or midazolam (overall aggregate mean Δarea under the curve-intracranial hypertension = +17 mm Hg × min, 95% CI, 0-34 mm Hg × min; p = 0.04). The mean Δarea under the curve-intracranial hypertension increased significantly after administration of high-dose fentanyl (p = 0.02), low-dose midazolam (p = 0.006), and high-dose fentanyl plus low-dose midazolam (0.007). Secondary analysis using age-dependent thresholds showed no significant impact on cerebral perfusion pressure deficit (mean Δarea under the curve-cerebral perfusion pressure).
Conclusions: Bolus dosing of fentanyl and midazolam fails to reduce the intracranial hypertension burden when administered for episodic intracranial hypertension. Paradoxically, we observed an overall increase in intracranial hypertension burden following drug administration, even after accounting for within-subject effects and time after injury. Future work is needed to confirm these findings in a prospective study design.
Conflict of interest statement
COPYRIGHT FORM DISCLOSURES: The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Analgesia, Sedation, and Intracranial Pressure: Questioning Our Approach in Pediatric Traumatic Brain Injury.Crit Care Med. 2016 Apr;44(4):851-2. doi: 10.1097/CCM.0000000000001679. Crit Care Med. 2016. PMID: 26974451 Free PMC article. No abstract available.
Similar articles
-
Effectiveness of Pharmacological Therapies for Intracranial Hypertension in Children With Severe Traumatic Brain Injury--Results From an Automated Data Collection System Time-Synched to Drug Administration.Pediatr Crit Care Med. 2016 Mar;17(3):236-45. doi: 10.1097/PCC.0000000000000610. Pediatr Crit Care Med. 2016. PMID: 26673840 Free PMC article.
-
Intracranial Hypertension and Cerebral Hypoperfusion in Children With Severe Traumatic Brain Injury: Thresholds and Burden in Accidental and Abusive Insults.Pediatr Crit Care Med. 2016 May;17(5):444-50. doi: 10.1097/PCC.0000000000000709. Pediatr Crit Care Med. 2016. PMID: 27028792 Free PMC article.
-
High-dose barbiturates for refractory intracranial hypertension in children with severe traumatic brain injury.Pediatr Crit Care Med. 2013 Mar;14(3):239-47. doi: 10.1097/PCC.0b013e318271c3b2. Pediatr Crit Care Med. 2013. PMID: 23392360
-
Comparison of the safety and efficacy of propofol with midazolam for sedation of patients with severe traumatic brain injury: a meta-analysis.J Crit Care. 2014 Apr;29(2):287-90. doi: 10.1016/j.jcrc.2013.10.021. Epub 2013 Oct 30. J Crit Care. 2014. PMID: 24360821 Review.
-
A Comparison of Pharmacologic Therapeutic Agents Used for the Reduction of Intracranial Pressure After Traumatic Brain Injury.World Neurosurg. 2017 Oct;106:509-528. doi: 10.1016/j.wneu.2017.07.009. Epub 2017 Jul 14. World Neurosurg. 2017. PMID: 28712906 Review.
Cited by
-
Acute Effects of Ketamine on Intracranial Pressure in Children With Severe Traumatic Brain Injury.Crit Care Med. 2023 May 1;51(5):563-572. doi: 10.1097/CCM.0000000000005806. Epub 2023 Feb 21. Crit Care Med. 2023. PMID: 36825892 Free PMC article.
-
Analgosedation in paediatric severe traumatic brain injury (TBI): practice, pitfalls and possibilities.Childs Nerv Syst. 2017 Oct;33(10):1703-1710. doi: 10.1007/s00381-017-3520-0. Epub 2017 Sep 6. Childs Nerv Syst. 2017. PMID: 29149387 Free PMC article. Review.
-
Pulmonary complications and respiratory management in neurocritical care: a narrative review.Chin Med J (Engl). 2022 Apr 5;135(7):779-789. doi: 10.1097/CM9.0000000000001930. Chin Med J (Engl). 2022. PMID: 35671179 Free PMC article. Review.
-
[Explanation and interpretation of blood transfusion provisions for critically ill and severely bleeding pediatric patients in the national health standard "Guideline for pediatric transfusion"].Zhongguo Dang Dai Er Ke Za Zhi. 2025 Apr 15;27(4):395-403. doi: 10.7499/j.issn.1008-8830.2501073. Zhongguo Dang Dai Er Ke Za Zhi. 2025. PMID: 40241356 Free PMC article. Chinese.
-
Clinical guidelines for traumatic brain injuries in children and boys.Eur J Transl Myol. 2020 Apr 1;30(1):8613. doi: 10.4081/ejtm.2019.8613. eCollection 2020 Apr 7. Eur J Transl Myol. 2020. PMID: 32499878 Free PMC article.
References
-
- Langlois JA, Rutland-Brown W, Thomas KE. The incidence of traumatic brain injury among children in the United States: differences by race. J Head Trauma Rehabil. 2005;20(3):229–238. - PubMed
-
- Schneier AJ, Shields BJ, Hostetler SG, Xiang H, Smith GA. Incidence of pediatric traumatic brain injury and associated hospital resource utilization in the United States. Pediatrics. 2006;118(2):483–492. - PubMed
-
- Adelson PD, Bratton SL, Carney NA, Chesnut RM, du Coudray HE, Goldstein B, Kochanek PM, Miller HC, Partington MD, Selden NR, et al. Guidelines for the acute medical management of severe traumatic brain injury in infants, children, and adolescents. Chapter 6. Threshold for treatment of intracranial hypertension. Pediatr Crit Care Med. 2003;4(3 Suppl):S25–S27. - PubMed
-
- Kochanek PM, Carney N, Adelson PD, Ashwal S, Bell MJ, Bratton S, Carson S, Chesnut RM, Ghajar J, Goldstein B, et al. Guidelines for the acute medical management of severe traumatic brain injury in infants, children, and adolescents--second edition. Pediatr Crit Care Med. 2012;13(Suppl 1):S1–S82. - PubMed
-
- Adelson PD, Bratton SL, Carney NA, Chesnut RM, du Coudray HE, Goldstein B, Kochanek PM, Miller HC, Partington MD, Selden NR, et al. Guidelines for the acute medical management of severe traumatic brain injury in infants, children, and adolescents. Chapter 8. Cerebral perfusion pressure. Pediatr Crit Care Med. 2003;4(3 Suppl):S31–S33. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
