

Nonhematopoietic Peroxisome Proliferator-Activated Receptor-α Protects Against Cardiac Injury and Enhances Survival in Experimental Polymicrobial Sepsis
- PMID: 26757163
- PMCID: PMC4940302
- DOI: 10.1097/CCM.0000000000001585
Nonhematopoietic Peroxisome Proliferator-Activated Receptor-α Protects Against Cardiac Injury and Enhances Survival in Experimental Polymicrobial Sepsis
Abstract
Objectives: Peroxisome proliferator-activated receptor-α is significantly down-regulated in circulating leukocytes from children with sepsis. Peroxisome proliferator-activated receptor-α null (Ppara) mice have greater mortality than wild-type mice when subjected to sepsis by cecal ligation and puncture. We sought to characterize the role of peroxisome proliferator-activated receptor-α in sepsis and to identify the mechanism whereby peroxisome proliferator-activated receptor-α confers a survival advantage.
Design: Prospective randomized preclinical study.
Setting: Laboratory investigation.
Subjects: Male C57Bl/6J and Ppara mice (B6.129S4-Ppara/J), aged 12-16 weeks.
Interventions: Bone marrow chimeric mice were generated and subjected to cecal ligation and puncture. Survival was measured for 7 days. Separate groups of nontransplanted mice underwent cecal ligation and puncture and were euthanized 24 hours later for plasma and tissue analyses.
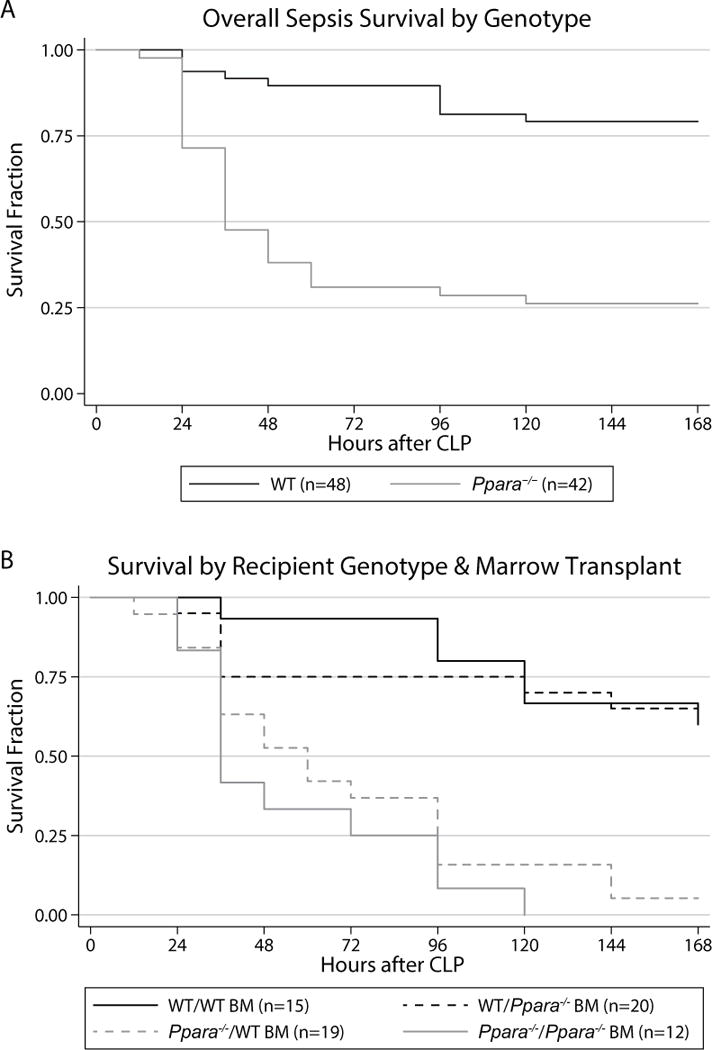
Measurements and main results: Ppara mice had dramatically reduced survival compared with wild-type mice irrespective of the peroxisome proliferator-activated receptor-α status of the bone marrow they received (3% vs 63%; p < 0.0001). No difference in survival was observed between Ppara mice that received wild-type versus Ppara marrow or in wild-type mice receiving wild-type versus Ppara marrow. In septic, nontransplanted mice at 24 hours, Ppara mice had elevated cardiac troponin levels compared with wild-type mice. Cardiac histologic injury scores were greater in Ppara versus wild-type mice. Expression of transcription factors and enzymes related to fatty acid oxidation in the heart were profoundly down-regulated in both wild-type and Ppara mice, but more so in the Ppara mice.
Conclusions: Peroxisome proliferator-activated receptor-α expression in nonhematopoietic tissues plays a critical role in determining clinical outcome in experimental polymicrobial sepsis and is more important to survival in sepsis than hematopoietic peroxisome proliferator-activated receptor-α expression. Cardiac injury due to inadequate energy production from fatty acid substrate is a probable mechanism of decreased survival in Ppara mice. These results suggest that altered peroxisome proliferator-activated receptor-α-mediated cellular metabolism may play an important role in sepsis-related end-organ injury and dysfunction, especially in the heart.
Conflict of interest statement
Conflicts of Interest: The remaining authors declared no conflicts of interest. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures






Comment in
-
The Molecular Complexity of Sepsis: Expression of Peroxisome Proliferator-Activated Receptor-α, the Tip of the Iceberg?Crit Care Med. 2016 Aug;44(8):1617-8. doi: 10.1097/CCM.0000000000001754. Crit Care Med. 2016. PMID: 27428127 No abstract available.
References
-
- Angus DC, van der Poll T. Severe Sepsis and Septic Shock. N Engl J Med. 2013;369:840–851. - PubMed
-
- Hartman ME, Linde-Zwirble WT, Angus DC, et al. Trends in the epidemiology of pediatric severe sepsis*. Pediatr Crit Care Med. 2013;14:686–693. - PubMed
-
- Lagu T, Rothberg MB, Shieh M-S, et al. Hospitalizations, costs, and outcomes of severe sepsis in the United States 2003 to 2007. Crit Care Med. 2012;40:754–761. - PubMed
-
- Ruth A, McCracken CE, Fortenberry JD, et al. Pediatric severe sepsis: current trends and outcomes from the pediatric health information systems database*. Pediatr Crit Care Med. 2014;15:828–838. - PubMed
-
- Angus DC. The search for effective therapy for sepsis: back to the drawing board? JAMA. 2011;306:2614–2615. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
