

Multinational Assessment of Accuracy of Equations for Predicting Risk of Kidney Failure: A Meta-analysis
- PMID: 26757465
- PMCID: PMC4752167
- DOI: 10.1001/jama.2015.18202
Multinational Assessment of Accuracy of Equations for Predicting Risk of Kidney Failure: A Meta-analysis
Erratum in
-
Incorrect Version Published.JAMA. 2016 Feb 23;315(8):822. doi: 10.1001/jama.2016.0342. JAMA. 2016. PMID: 26903348 No abstract available.
Abstract
Importance: Identifying patients at risk of chronic kidney disease (CKD) progression may facilitate more optimal nephrology care. Kidney failure risk equations, including such factors as age, sex, estimated glomerular filtration rate, and calcium and phosphate concentrations, were previously developed and validated in 2 Canadian cohorts. Validation in other regions and in CKD populations not under the care of a nephrologist is needed.
Objective: To evaluate the accuracy of the risk equations across different geographic regions and patient populations through individual participant data meta-analysis.
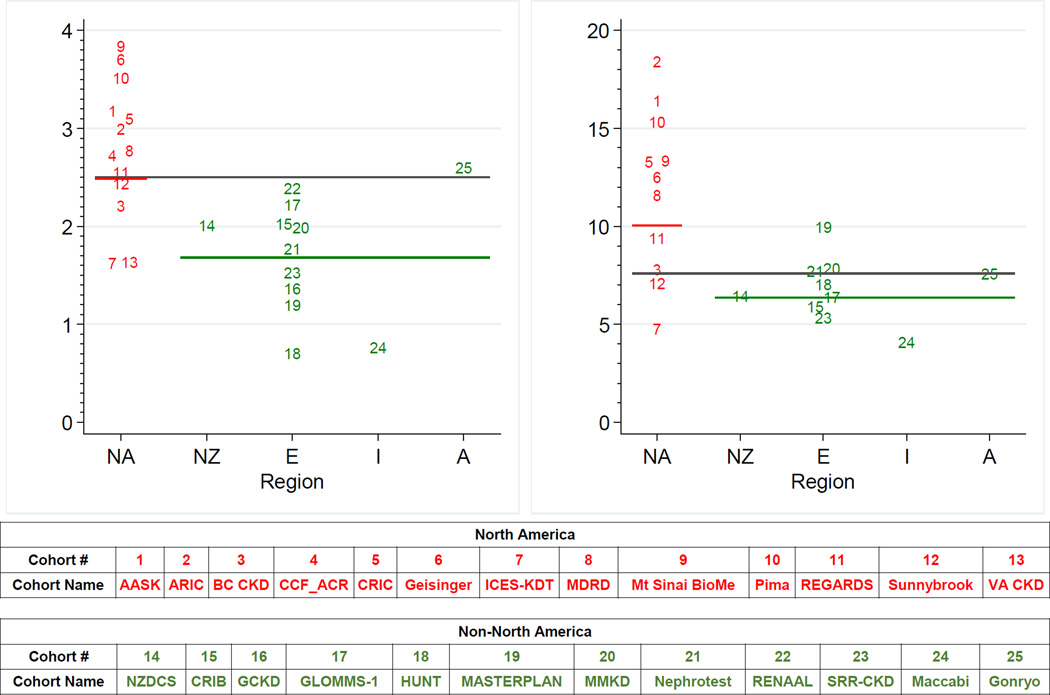
Data sources: Thirty-one cohorts, including 721,357 participants with CKD stages 3 to 5 in more than 30 countries spanning 4 continents, were studied. These cohorts collected data from 1982 through 2014.
Study selection: Cohorts participating in the CKD Prognosis Consortium with data on end-stage renal disease.
Data extraction and synthesis: Data were obtained and statistical analyses were performed between July 2012 and June 2015. Using the risk factors from the original risk equations, cohort-specific hazard ratios were estimated and combined using random-effects meta-analysis to form new pooled kidney failure risk equations. Original and pooled kidney failure risk equation performance was compared, and the need for regional calibration factors was assessed.
Main outcomes and measures: Kidney failure (treatment by dialysis or kidney transplant).
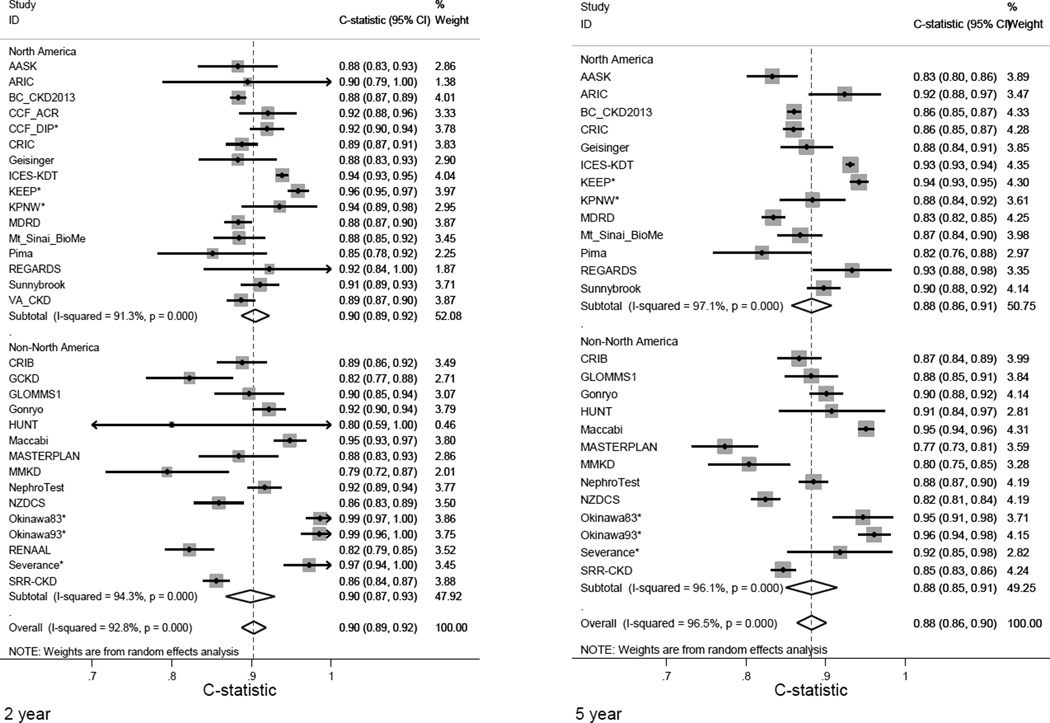
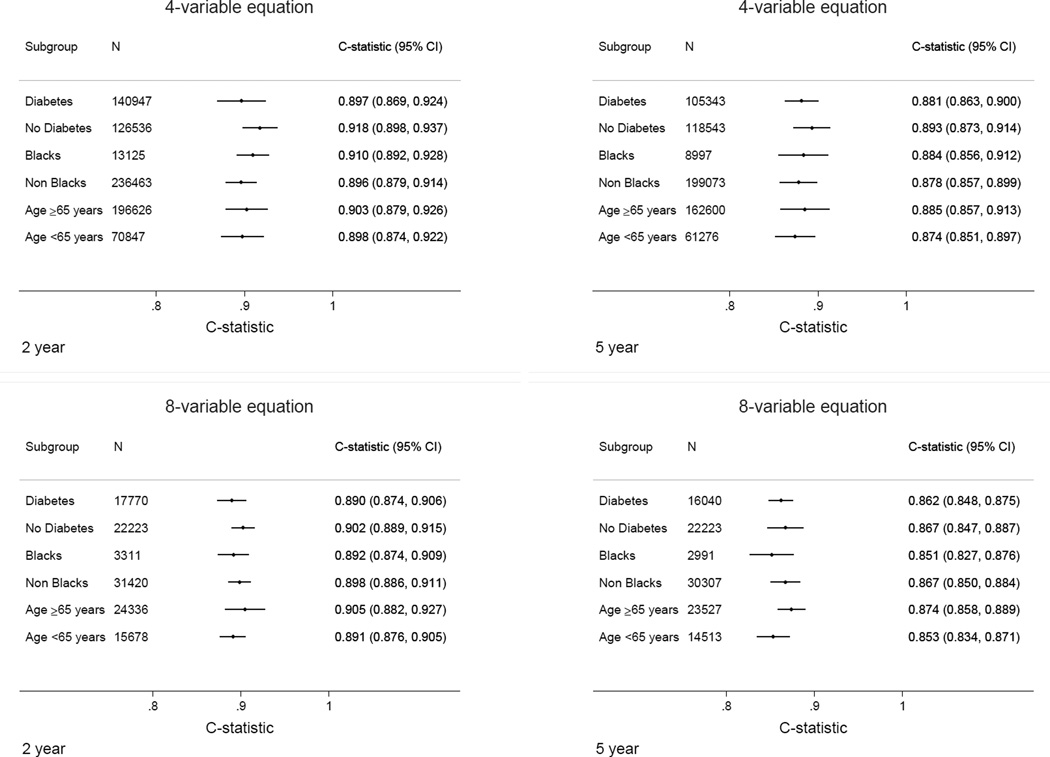
Results: During a median follow-up of 4 years of 721,357 participants with CKD, 23,829 cases kidney failure were observed. The original risk equations achieved excellent discrimination (ability to differentiate those who developed kidney failure from those who did not) across all cohorts (overall C statistic, 0.90; 95% CI, 0.89-0.92 at 2 years; C statistic at 5 years, 0.88; 95% CI, 0.86-0.90); discrimination in subgroups by age, race, and diabetes status was similar. There was no improvement with the pooled equations. Calibration (the difference between observed and predicted risk) was adequate in North American cohorts, but the original risk equations overestimated risk in some non-North American cohorts. Addition of a calibration factor that lowered the baseline risk by 32.9% at 2 years and 16.5% at 5 years improved the calibration in 12 of 15 and 10 of 13 non-North American cohorts at 2 and 5 years, respectively (P = .04 and P = .02).
Conclusions and relevance: Kidney failure risk equations developed in a Canadian population showed high discrimination and adequate calibration when validated in 31 multinational cohorts. However, in some regions the addition of a calibration factor may be necessary.
Conflict of interest statement
Figures
References
-
- Coresh J, Selvin E, Stevens LA, et al. Prevalence of chronic kidney disease in the United States. JAMA. 2007 Nov 7;298(17):2038–2047. - PubMed
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004 Sep 23;351(13):1296–1305. - PubMed
-
- O'Hare AM, Bertenthal D, Walter LC, et al. When to refer patients with chronic kidney disease for vascular access surgery: should age be a consideration? Kidney Int. 2007 Mar;71(6):555–561. - PubMed
-
- Tobe SW, Clase CM, Gao P, et al. Cardiovascular and renal outcomes with telmisartan, ramipril, or both in people at high renal risk: results from the ONTARGET and TRANSCEND studies. Circulation. 2011 Mar 15;123(10):1098–1107. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 DK061028/DK/NIDDK NIH HHS/United States
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- R01 CA165001/CA/NCI NIH HHS/United States
- K23 DK067303/DK/NIDDK NIH HHS/United States
- U01 DK035073/DK/NIDDK NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- U01 DK060984/DK/NIDDK NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- K23 DK002904/DK/NIDDK NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- U01 DK060980/DK/NIDDK NIH HHS/United States
- U01 DK060963/DK/NIDDK NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- K08DK092287/DK/NIDDK NIH HHS/United States
- U01 DK061022/DK/NIDDK NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- U01 NS041588/NS/NINDS NIH HHS/United States
- R01DK100446-01/DK/NIDDK NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- U01 DK060902/DK/NIDDK NIH HHS/United States
- U01 DK060990/DK/NIDDK NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- K08 DK092287/DK/NIDDK NIH HHS/United States
- R01 DK100446/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
