

Rationale and Early Experience with Prophylactic Placement of Mesh to Prevent Parastomal Hernia Formation after Ileal Conduit Urinary Diversion and Cystectomy for Bladder Cancer
- PMID: 26757903
- PMCID: PMC4803475
- DOI: 10.1007/s11934-015-0565-z
Rationale and Early Experience with Prophylactic Placement of Mesh to Prevent Parastomal Hernia Formation after Ileal Conduit Urinary Diversion and Cystectomy for Bladder Cancer
Abstract
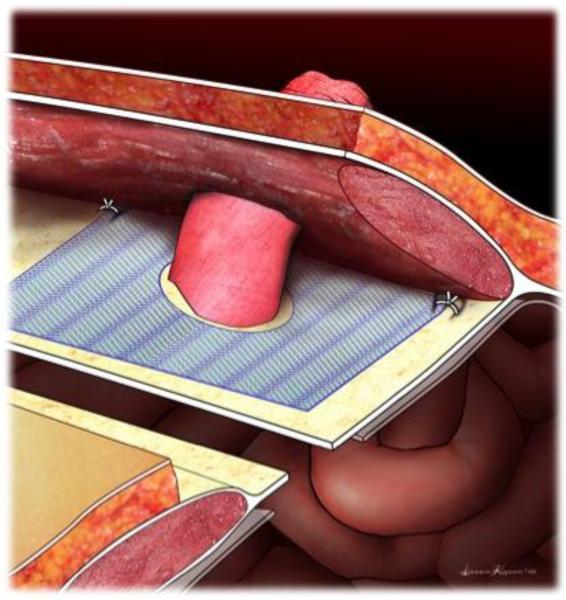
Parastomal hernias (PH) represent a clinically significant problem for many patients after radical cystectomy and ileal conduit diversion. The prevalence may be as high as 60% and in some series, up to 30% of patients require surgical intervention due to the complications of pain, poor fit of an ostomy appliance, leakage, urinary obstruction, and bowel obstruction or strangulation. Due to the potential morbidity associated with PH repair, there have been efforts to prevent PH development at the time of the index surgery. Four randomized trials of prophylactic mesh placement at the time of colostomy and ileostomy stoma formation have demonstrated significant reductions in PH rates with acceptably low complication rates. In this review, we describe the clinical and radiographic definitions of PH, the clinical impact and risk factors behind its development, and the rationale behind prophylactic mesh placement for patients undergoing ileal conduit urinary diversion. Additionally, we report our experience with prophylactic mesh placed at radical cystectomy at our institution.
Keywords: Ileal conduit; Parastomal hernia; Radical cystectomy.
Figures
Similar articles
-
Parastomal hernias after cystectomy and ileal conduit urinary diversion: surgical treatment and the use of prophylactic mesh: a systematic review.BMC Surg. 2022 Mar 29;22(1):118. doi: 10.1186/s12893-022-01509-y. BMC Surg. 2022. PMID: 35351086 Free PMC article.
-
Parastomal hernias after radical cystectomy and ileal conduit diversion.Investig Clin Urol. 2016 Jul;57(4):240-8. doi: 10.4111/icu.2016.57.4.240. Epub 2016 Jul 5. Investig Clin Urol. 2016. PMID: 27437533 Free PMC article. Review.
-
Prophylactic mesh used in ileal conduit formation following radical cystectomy: a retrospective cohort.Hernia. 2018 Oct;22(5):781-784. doi: 10.1007/s10029-018-1801-5. Epub 2018 Aug 10. Hernia. 2018. PMID: 30097796
-
Prophylactic Parastomal Mesh Sublay at the Time of Ileal Conduit: Surgical Technique.Urology. 2022 Nov;169:269-271. doi: 10.1016/j.urology.2022.07.022. Epub 2022 Jul 28. Urology. 2022. PMID: 35907483
-
Natural History and Predictors of Parastomal Hernia after Robot-Assisted Radical Cystectomy and Ileal Conduit Urinary Diversion.J Urol. 2018 Mar;199(3):766-773. doi: 10.1016/j.juro.2017.08.112. Epub 2017 Sep 7. J Urol. 2018. PMID: 28890392
Cited by
-
Parastomal hernias after cystectomy and ileal conduit urinary diversion: surgical treatment and the use of prophylactic mesh: a systematic review.BMC Surg. 2022 Mar 29;22(1):118. doi: 10.1186/s12893-022-01509-y. BMC Surg. 2022. PMID: 35351086 Free PMC article.
-
Assessment of Urostomy Parastomal Herniation Forces Using Incisional Prevention Strategies with an Abdominal Fascia Model.Eur Urol Open Sci. 2023 Jun 21;54:66-71. doi: 10.1016/j.euros.2023.05.019. eCollection 2023 Aug. Eur Urol Open Sci. 2023. PMID: 37485469 Free PMC article.
-
Ileal conduit or orthotopic neobladder: selection and contemporary patterns of use.Curr Opin Urol. 2020 May;30(3):415-420. doi: 10.1097/MOU.0000000000000738. Curr Opin Urol. 2020. PMID: 32141937 Free PMC article. Review.
-
Prophylactic Mesh in Parastomal Hernia Prevention: Current Evidence.J Abdom Wall Surg. 2025 Jul 30;4:15011. doi: 10.3389/jaws.2025.15011. eCollection 2025. J Abdom Wall Surg. 2025. PMID: 40808717 Free PMC article. Review.
-
Keyhole versus Sugarbaker techniques in parastomal hernia repair following ileal conduit urinary diversion: a retrospective nationwide cohort study.BMC Surg. 2021 May 3;21(1):231. doi: 10.1186/s12893-021-01228-w. BMC Surg. 2021. PMID: 33941154 Free PMC article.
References
-
- Pearl RK. Parastomal hernias. World J Surg. 1989;13:569. - PubMed
-
- Israelsson LA. Parastomal hernias. Surg Clin North Am. 2008;88:113. - PubMed
-
- Gerharz EW, Mansson A, Hunt S, et al. Quality of life after cystectomy and urinary diversion: an evidence based analysis. J Urol. 2005;174:1729. - PubMed
-
- Kouba E, Sands M, Lentz A, et al. Incidence and risk factors of stomal complications in patients undergoing cystectomy with ileal conduit urinary diversion for bladder cancer. J Urol. 2007;178:950. - PubMed
-
- Goligher JC, Lloyd-Davies OV, Robertson CT. Small-gut obstructions following combined excision of the rectum with special reference to strangulation round the colostomy. Br J Surg. 1951;38:467. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
