

Genomic complexity of urothelial bladder cancer revealed in urinary cfDNA
- PMID: 26757983
- PMCID: PMC4970693
- DOI: 10.1038/ejhg.2015.281
Genomic complexity of urothelial bladder cancer revealed in urinary cfDNA
Abstract
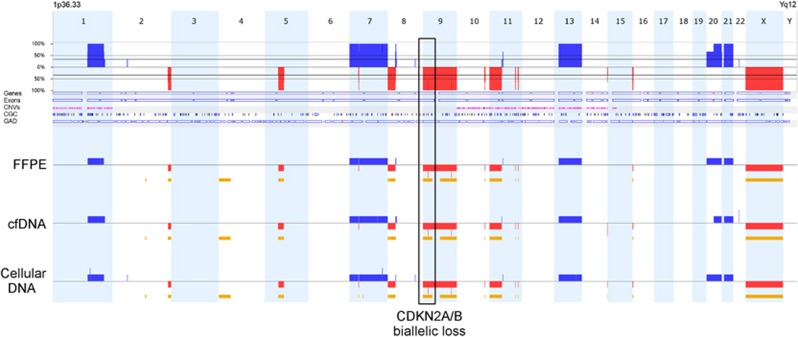
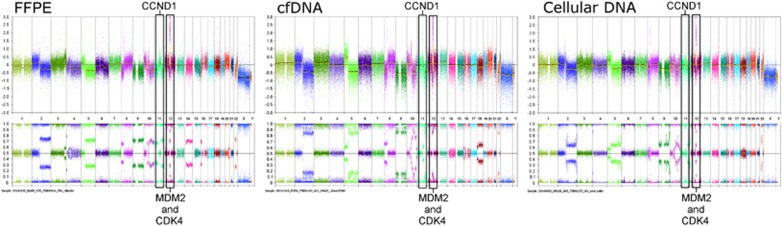
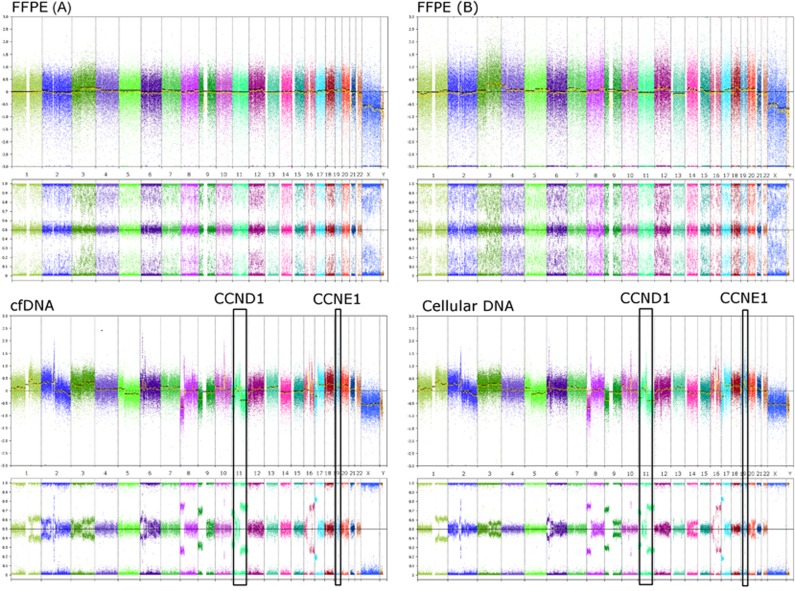
Urothelial bladder cancers (UBCs) have heterogeneous clinical characteristics that are mirrored in their diverse genomic profiles. Genomic profiling of UBCs has the potential to benefit routine clinical practice by providing prognostic utility above and beyond conventional clinicopathological factors, and allowing for prediction and surveillance of treatment responses. Urinary DNAs representative of the tumour genome provide a promising resource as a liquid biopsy for non-invasive genomic profiling of UBCs. We compared the genomic profiles of urinary cellular DNA and cell-free DNA (cfDNA) from the urine with matched diagnostic formalin-fixed paraffin-embedded tumour DNAs for 23 well-characterised UBC patients. Our data show urinary DNAs to be highly representative of patient tumours, allowing for detection of recurrent clinically actionable genomic aberrations. Furthermore, a greater aberrant load (indicative of tumour genome) was observed in cfDNA over cellular DNA (P<0.001), resulting in a higher analytical sensitivity for detection of clinically actionable genomic aberrations (P<0.04) when using cfDNA. Thus, cfDNA extracted from the urine of UBC patients has a higher tumour genome burden and allows greater detection of key genomic biomarkers (90%) than cellular DNA from urine (61%) and provides a promising resource for robust whole-genome tumour profiling of UBC with potential to influence clinical decisions without invasive patient interventions.
Conflict of interest statement
RTB has previously contributed to an advisory board for Olympus Medical Systems with regard to narrow band imaging cystoscopy. JMF, AO and KGS are all paid employees of Affymetrix UK Ltd and hold shares in Affymetrix (NASDAQ: AFFX). The remaining authors declare no conflict of interest.
Figures
References
-
- Schrier BP, Hollander MP, van Rhijn BWG, Kiemeney LALM, Witjes JA: Prognosis of muscle-invasive bladder cancer: difference between primary and progressive tumours and implications for therapy. Eur Urol 2004; 45: 292–296. - PubMed
-
- Moschini M, Sharma V, Dell'oglio P, Cucchiara V, Gandaglia G, Cantiello F et al: Comparing long-term outcomes between primary versus progressive muscle invasive bladder cancer after radical cystectomy. BJU Int 2015, e-pub ahead of print 7 April 2015; doi:10.1111/bju.13146. - PubMed
-
- Witjes JA, Compérat E, Cowan NC, De Santis M, Gakis G, Lebret T et al: EAU guidelines on muscle-invasive and metastatic bladder cancer: summary of the 2013 guidelines. Eur Urol 2014; 65: 778–792. - PubMed
-
- Knowles MA, Hurst CD: Molecular biology of bladder cancer: new insights into pathogenesis and clinical diversity. Nat Rev Cancer 2014; 15: 25–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
