

Cost-effectiveness analysis of arthroscopic surgery compared with non-operative management for osteoarthritis of the knee
- PMID: 26758265
- PMCID: PMC4716206
- DOI: 10.1136/bmjopen-2015-009949
Cost-effectiveness analysis of arthroscopic surgery compared with non-operative management for osteoarthritis of the knee
Abstract
Objective: To determine the cost-effectiveness of arthroscopic surgery in addition to non-operative treatments compared with non-operative treatments alone in patients with knee osteoarthritis (OA).
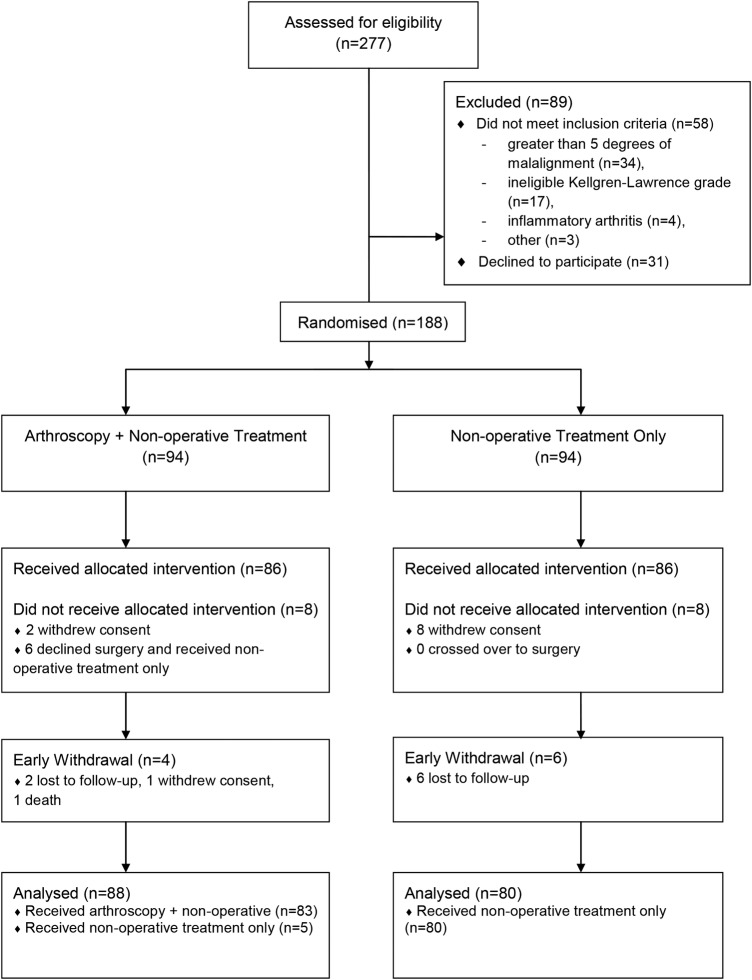
Design, setting and participants: We conducted an economic evaluation alongside a single-centre, randomised trial among patients with symptomatic, radiographic knee OA (KL grade ≥ 2).
Interventions: Patients received arthroscopic debridement and partial resection of degenerative knee tissues in addition to optimised non-operative therapy, or optimised non-operative therapy only.
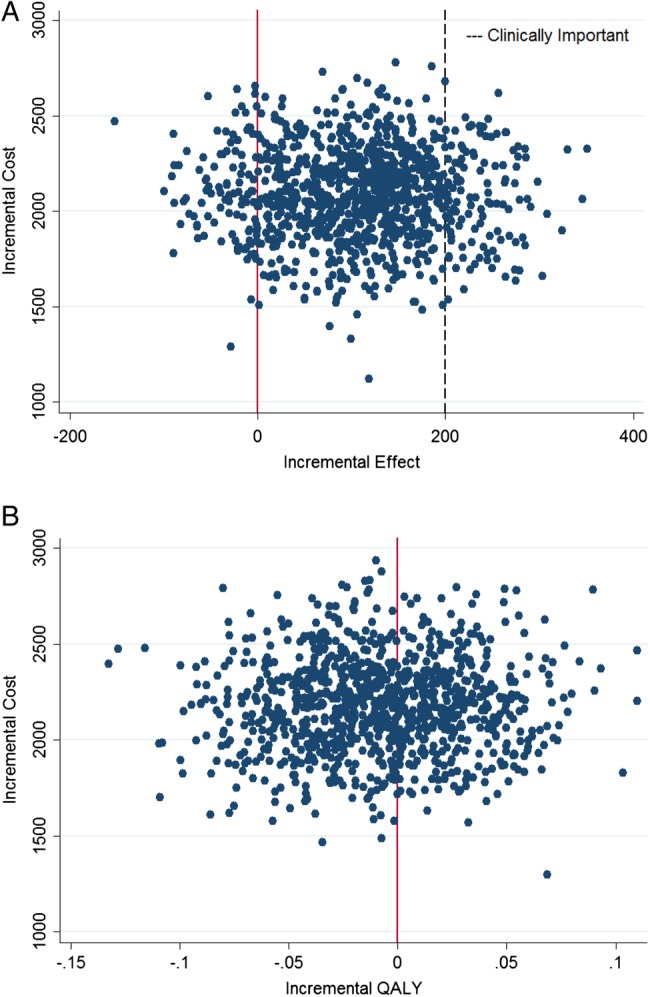
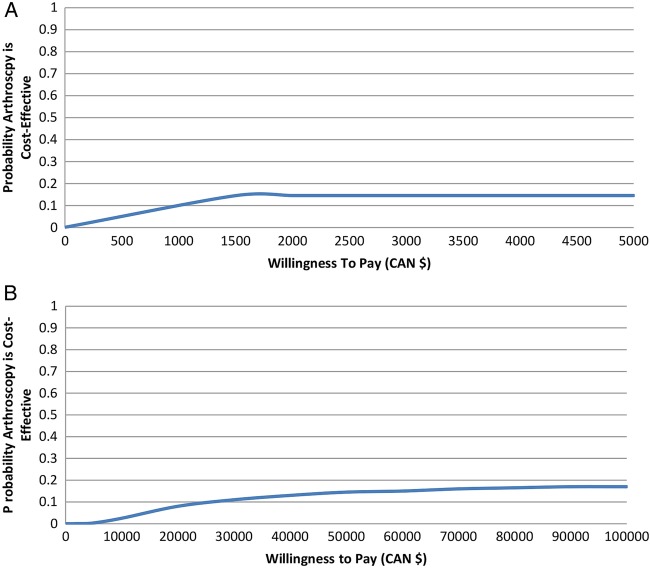
Main outcome measures: Direct and indirect costs were collected prospectively over the 2-year study period. The effectiveness outcomes were the Western Ontario McMaster Osteoarthritis Index (WOMAC) and quality-adjusted life years (QALYs). Cost-effectiveness was estimated using the net benefit regression framework considering a range of willingness-to-pay values from the Canadian public payer and societal perspectives. We calculated incremental cost-effectiveness ratios and conducted sensitivity analyses using the extremes of the 95% CIs surrounding mean differences in effect between groups.
Results: 168 patients were included. Patients allocated to arthroscopy received partial resection and debridement of degenerative meniscal tears (81%) and/or articular cartilage (97%). There were no significant differences between groups in use of non-operative treatments. The incremental net benefit was negative for all willingness-to-pay values. Uncertainty estimates suggest that even if willing to pay $400,000 to achieve a clinically important improvement in WOMAC score, or ≥$50,000 for an additional QALY, there is <20% probability that the addition of arthroscopy is cost-effective compared with non-operative therapies only. Our sensitivity analysis suggests that even when assuming the largest treatment effect, the addition of arthroscopic surgery is not economically attractive compared with non-operative treatments only.
Conclusions: Arthroscopic debridement of degenerative articular cartilage and resection of degenerative meniscal tears in addition to non-operative treatments for knee OA is not an economically attractive treatment option compared with non-operative treatment only, regardless of willingness-to-pay value.
Trial registration number: NCT00158431.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical