

Pathophysiology and treatment of pulmonary hypertension in sickle cell disease
- PMID: 26758918
- PMCID: PMC4760088
- DOI: 10.1182/blood-2015-08-618561
Pathophysiology and treatment of pulmonary hypertension in sickle cell disease
Abstract
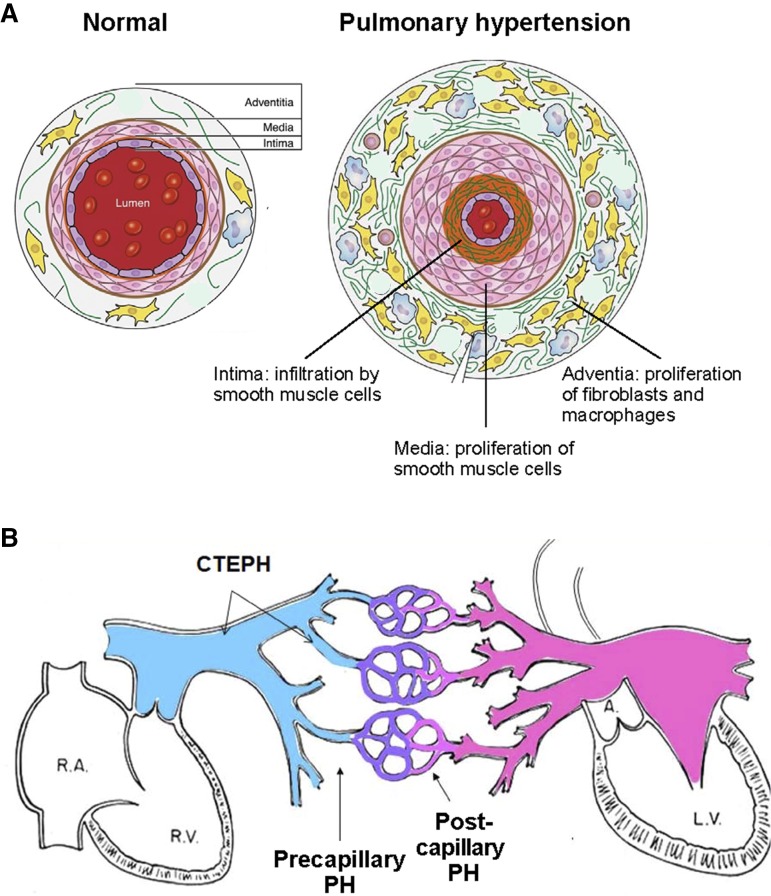
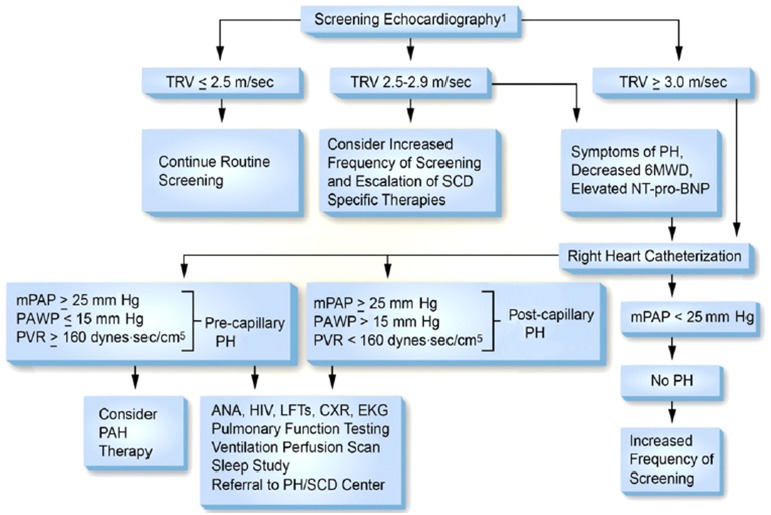
Pulmonary hypertension affects ∼10% of adult patients with sickle cell disease (SCD), particularly those with the homozygous genotype. An increase in pulmonary artery systolic pressure, estimated noninvasively by echocardiography, helps identify SCD patients at risk for pulmonary hypertension, but definitive diagnosis requires right-heart catheterization. About half of SCD-related pulmonary hypertension patients have precapillary pulmonary hypertension with potential etiologies of (1) a nitric oxide deficiency state and vasculopathy consequent to intravascular hemolysis, (2) chronic pulmonary thromboembolism, or (3) upregulated hypoxic responses secondary to anemia, low O2 saturation, and microvascular obstruction. The remainder have postcapillary pulmonary hypertension secondary to left ventricular dysfunction. Although the pulmonary artery pressure in SCD patients with pulmonary hypertension is only moderately elevated, they have a markedly higher risk of death than patients without pulmonary hypertension. Guidelines for diagnosis and management of SCD-related pulmonary hypertension were published recently by the American Thoracic Society. Management of adults with sickle-related pulmonary hypertension is based on anticoagulation for those with thromboembolism; oxygen therapy for those with low oxygen saturation; treatment of left ventricular failure in those with postcapillary pulmonary hypertension; and hydroxyurea or transfusions to raise the hemoglobin concentration, reduce hemolysis, and prevent vaso-occlusive events that cause additional increases in pulmonary pressure. Randomized trials have not identified drugs to lower pulmonary pressure in SCD patients with precapillary pulmonary hypertension. Patients with hemodynamics of pulmonary arterial hypertension should be referred to specialized centers and considered for treatments known to be effective in other forms of pulmonary arterial hypertension. There have been reports that some of these treatments improve SCD-related pulmonary hypertension.
© 2016 by The American Society of Hematology.
Figures
Similar articles
-
An official American Thoracic Society clinical practice guideline: diagnosis, risk stratification, and management of pulmonary hypertension of sickle cell disease.Am J Respir Crit Care Med. 2014 Mar 15;189(6):727-40. doi: 10.1164/rccm.201401-0065ST. Am J Respir Crit Care Med. 2014. PMID: 24628312 Free PMC article.
-
Sickle cell disease: at the crossroads of pulmonary hypertension and diastolic heart failure.Heart. 2020 Apr;106(8):562-568. doi: 10.1136/heartjnl-2019-314810. Epub 2019 Dec 10. Heart. 2020. PMID: 31822569 Free PMC article. Review.
-
Hypoxic response contributes to altered gene expression and precapillary pulmonary hypertension in patients with sickle cell disease.Circulation. 2014 Apr 22;129(16):1650-8. doi: 10.1161/CIRCULATIONAHA.113.005296. Epub 2014 Feb 10. Circulation. 2014. PMID: 24515990 Free PMC article.
-
Nitric Oxide-Independent Soluble Guanylate Cyclase Activation Improves Vascular Function and Cardiac Remodeling in Sickle Cell Disease.Am J Respir Cell Mol Biol. 2018 May;58(5):636-647. doi: 10.1165/rcmb.2017-0292OC. Am J Respir Cell Mol Biol. 2018. PMID: 29268036 Free PMC article.
-
Sickle cell anemia-associated pulmonary arterial hypertension.J Bras Pneumol. 2007 Sep-Oct;33(5):583-91. doi: 10.1590/s1806-37132007000500015. J Bras Pneumol. 2007. PMID: 18026658 Review. English, Portuguese.
Cited by
-
Exercise-induced changes of vital signs in adults with sickle cell disease.Am J Hematol. 2021 Dec 1;96(12):1630-1638. doi: 10.1002/ajh.26369. Epub 2021 Oct 20. Am J Hematol. 2021. PMID: 34626431 Free PMC article. Clinical Trial.
-
Evidence supporting a role for circulating macrophages in the regression of vascular remodeling following sub-chronic exposure to hemoglobin plus hypoxia.Pulm Circ. 2021 Nov 5;11(4):20458940211056806. doi: 10.1177/20458940211056806. eCollection 2021 Oct-Dec. Pulm Circ. 2021. PMID: 34777787 Free PMC article.
-
Depletion of haptoglobin and hemopexin promote hemoglobin-mediated lipoprotein oxidation in sickle cell disease.Am J Physiol Lung Cell Mol Physiol. 2018 Nov 1;315(5):L765-L774. doi: 10.1152/ajplung.00269.2018. Epub 2018 Jul 26. Am J Physiol Lung Cell Mol Physiol. 2018. PMID: 30047285 Free PMC article.
-
Tricuspid regurgitation velocity and other biomarkers of mortality in children, adolescents and young adults with sickle cell disease in the United States: The PUSH study.Am J Hematol. 2020 Jul;95(7):766-774. doi: 10.1002/ajh.25799. Epub 2020 Apr 21. Am J Hematol. 2020. PMID: 32243618 Free PMC article. Clinical Trial.
-
Improving prognostic evaluations in patients with stage IIIb light chain cardiac amyloidosis: role of haemodynamic parameters.Orphanet J Rare Dis. 2025 Jan 13;20(1):19. doi: 10.1186/s13023-024-03451-z. Orphanet J Rare Dis. 2025. PMID: 39806404 Free PMC article.
References
-
- Rees DC, Williams TN, Gladwin MT. Sickle-cell disease. Lancet. 2010;376(9757):2018–2031. - PubMed
-
- Badesch DB, Champion HC, Sanchez MA, et al. Diagnosis and assessment of pulmonary arterial hypertension. J Am Coll Cardiol. 2009;54(1 Suppl):S55–S66. - PubMed
-
- Hoeper MM, Bogaard HJ, Condliffe R, et al. Definitions and diagnosis of pulmonary hypertension. J Am Coll Cardiol. 2013;62(25 Suppl):D42–D50. - PubMed
-
- Galiè N, Hoeper MM, Humbert M, et al. Task Force for Diagnosis and Treatment of Pulmonary Hypertension of European Society of Cardiology (ESC); European Respiratory Society (ERS); International Society of Heart and Lung Transplantation (ISHLT) Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J. 2009;34(6):1219–1263. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
