

Ischemic penumbra as a trigger for intracranial pressure rise - A potential cause for collateral failure and infarct progression?
- PMID: 26759431
- PMCID: PMC4853839
- DOI: 10.1177/0271678X15625578
Ischemic penumbra as a trigger for intracranial pressure rise - A potential cause for collateral failure and infarct progression?
Abstract
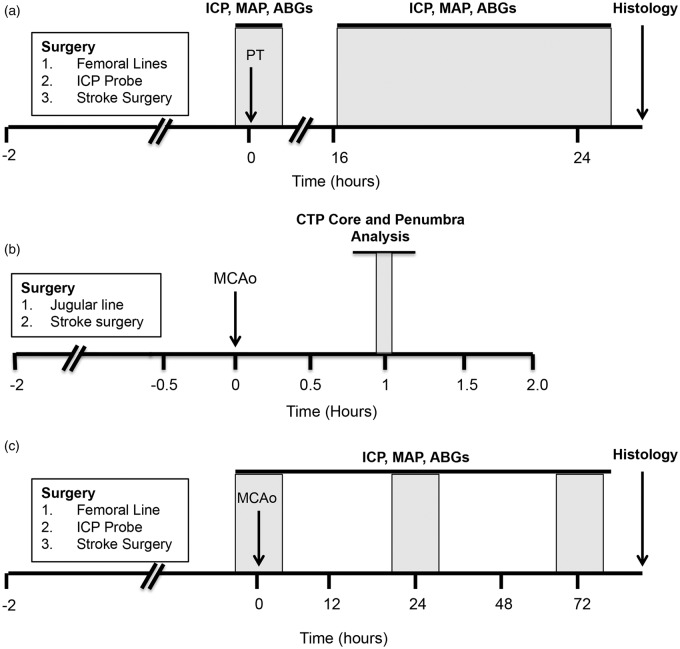
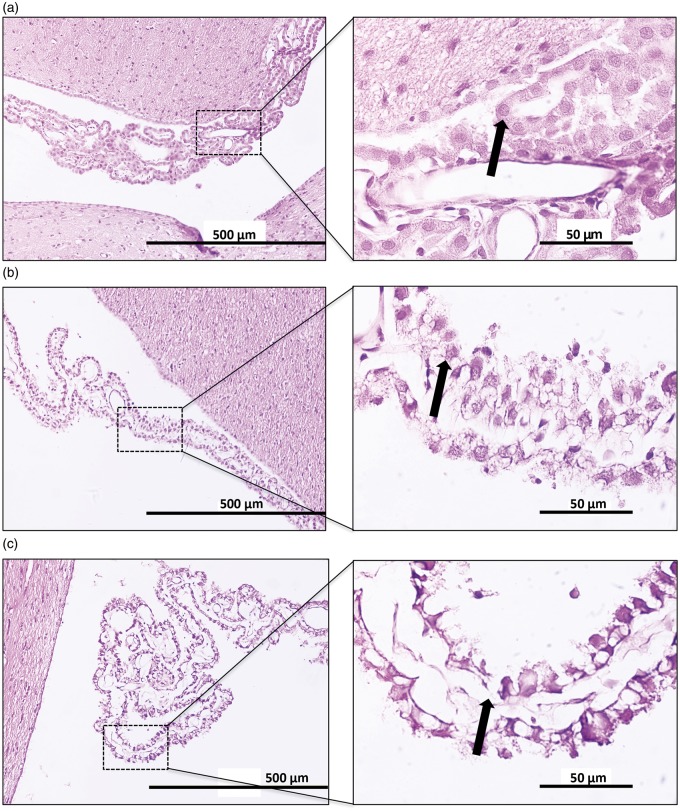
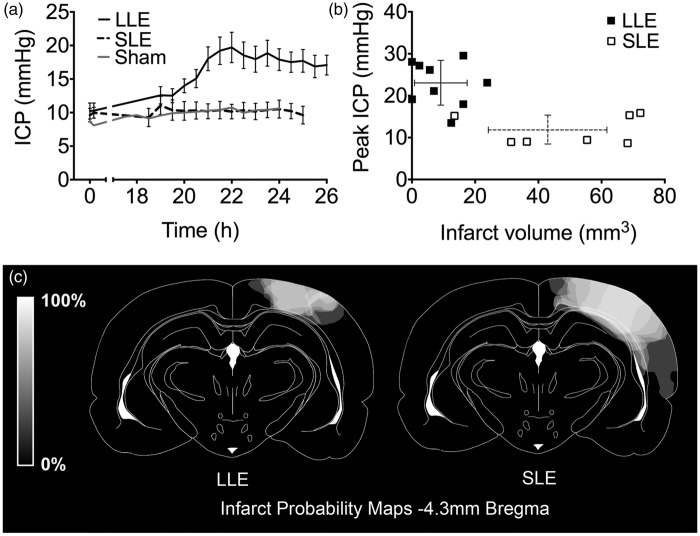
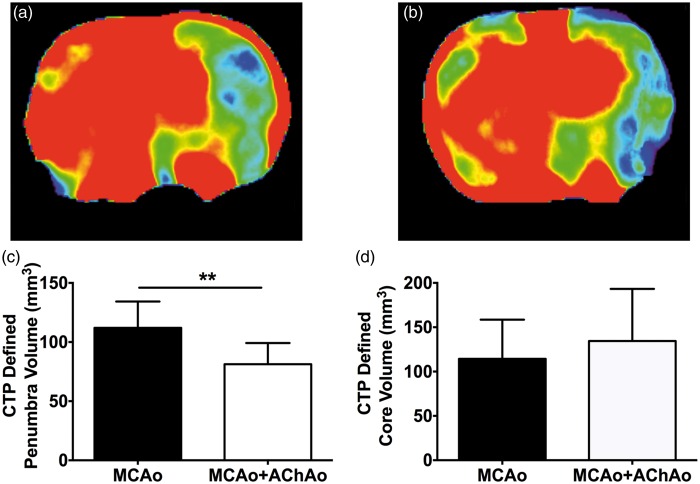
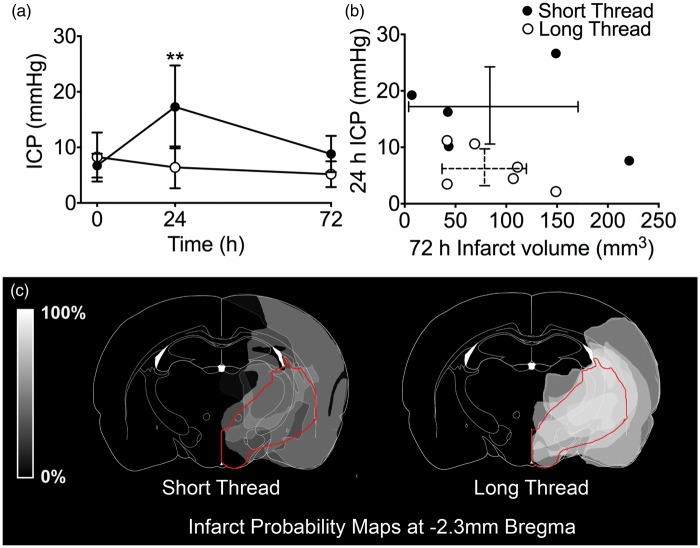
We have recently shown that intracranial pressure (ICP) increases dramatically 24 h after minor intraluminal thread occlusion with reperfusion, independent of edema. Some of the largest ICP rises were observed in rats with the smallest final infarcts. A possible alternate mechanism for this ICP rise is an increase of cerebrospinal fluid (CSF) volume secondary to choroid plexus damage (a known complication of the intraluminal stroke model used). Alternatively, submaximal injury may be needed to induce ICP elevation. Therefore, we aimed to determine (a) if choroid plexus damage contributes to the ICP elevation, (b) if varying the patency of an important internal collateral supply to the middle cerebral artery (MCA), the anterior choroidal artery (AChA), produces different volumes of ischemic penumbra and (c) if presence of ischemic penumbra (submaximal injury) is associated with ICP elevation. We found (a) no association between choroid plexus damage and ICP elevation, (b) animals with a good internal collateral supply through the AChA during MCAo had significantly larger penumbra volumes and (c) ICP elevation at ≈24 h post-stroke only occurred in rats with submaximal injury, shown in two different stroke models. We conclude that active cellular processes within the ischemic penumbra may be required for edema-independent ICP elevation.
Keywords: Collaterals; intracranial pressure; middle cerebral artery occlusion; penumbra; photothrombosis.
© The Author(s) 2016.
Figures
References
-
- Murtha LA, McLeod DD, McCann SK, et al. Short-duration hypothermia after ischemic stroke prevents delayed intracranial pressure rise. Int J Stroke 2014; 9: 553–559. - PubMed
-
- Ennis SR, Keep RF. The effects of cerebral ischemia on the rat choroid plexus. J Cereb Blood Flow Metab 2006; 26: 675–683. - PubMed
-
- Coutts SB, Modi J, Patel SK, et al. CT/CT angiography and MRI findings predict recurrent stroke after transient ischemic attack and minor stroke: results of the prospective CATCH study. Stroke 2012; 43: 1013–1017. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
