

Risk Factors for Cutaneous Squamous Cell Carcinoma Recurrence, Metastasis, and Disease-Specific Death: A Systematic Review and Meta-analysis
- PMID: 26762219
- PMCID: PMC4833641
- DOI: 10.1001/jamadermatol.2015.4994
Risk Factors for Cutaneous Squamous Cell Carcinoma Recurrence, Metastasis, and Disease-Specific Death: A Systematic Review and Meta-analysis
Abstract
Importance: To date, the magnitude of association and the quality of evidence for cutaneous squamous cell carcinoma (cSCC) and risk factors for outcomes have not been reviewed and analyzed systematically.
Objective: To systematically analyze all published data on risk factors for recurrence, metastasis, and disease-specific death (DSD) of cSCC.
Data sources: Comprehensive search of Ovid MEDLINE In-Process & Other Non-Indexed Citations, MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, and Scopus, from each database's inception to May 14, 2015.
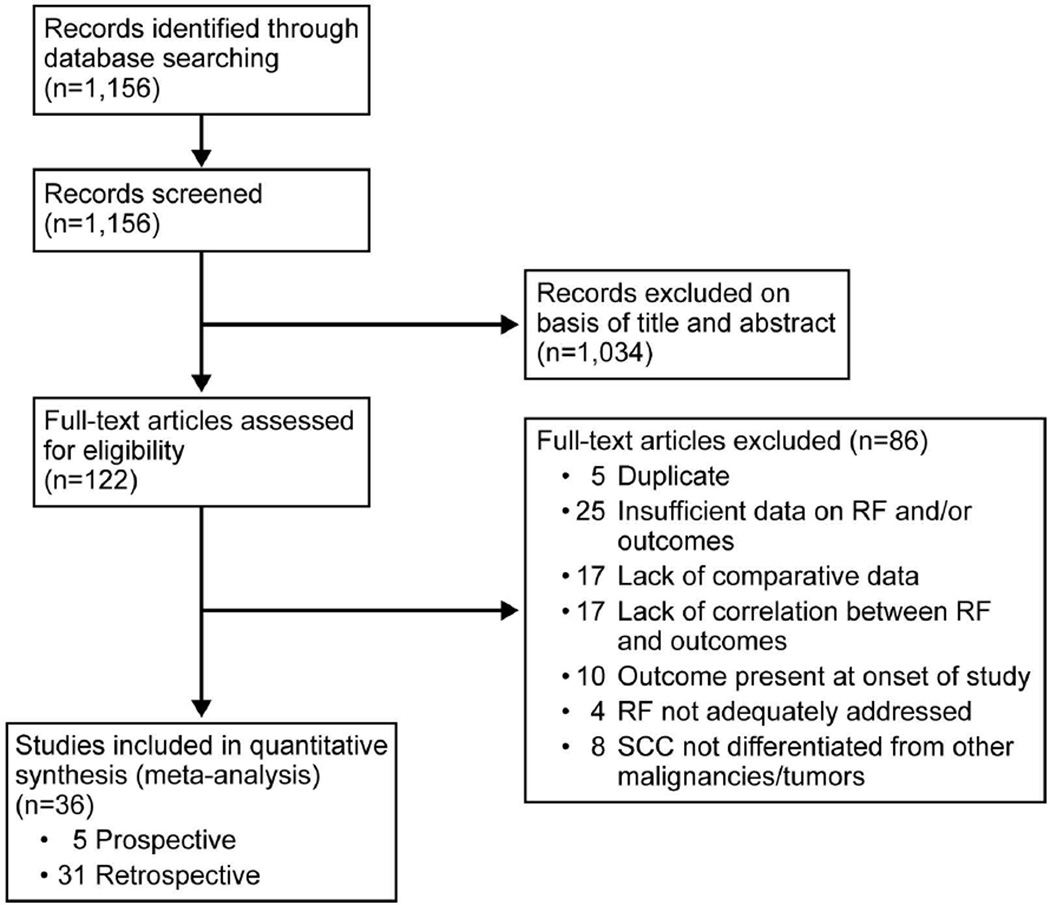
Study selection: Inclusion criteria were studies of at least 10 patients, comparative data for at least 1 cSCC risk factor, and an outcome of interest. Exclusion criteria were noncutaneous squamous cell carcinoma (SCC), anogenital SCC, inability to extract cSCC data from other malignancy data, SCC in situ, Marjolin ulcer, and genetic disorders predisposing to cSCC.
Data extraction and synthesis: Two reviewers independently abstracted the data. Meta-analysis was performed using the random-effects model. Risk of bias was assessed by the Newcastle-Ottawa Scale.
Main outcomes and measures: A priori outcomes were recurrence, metastasis, and DSD.
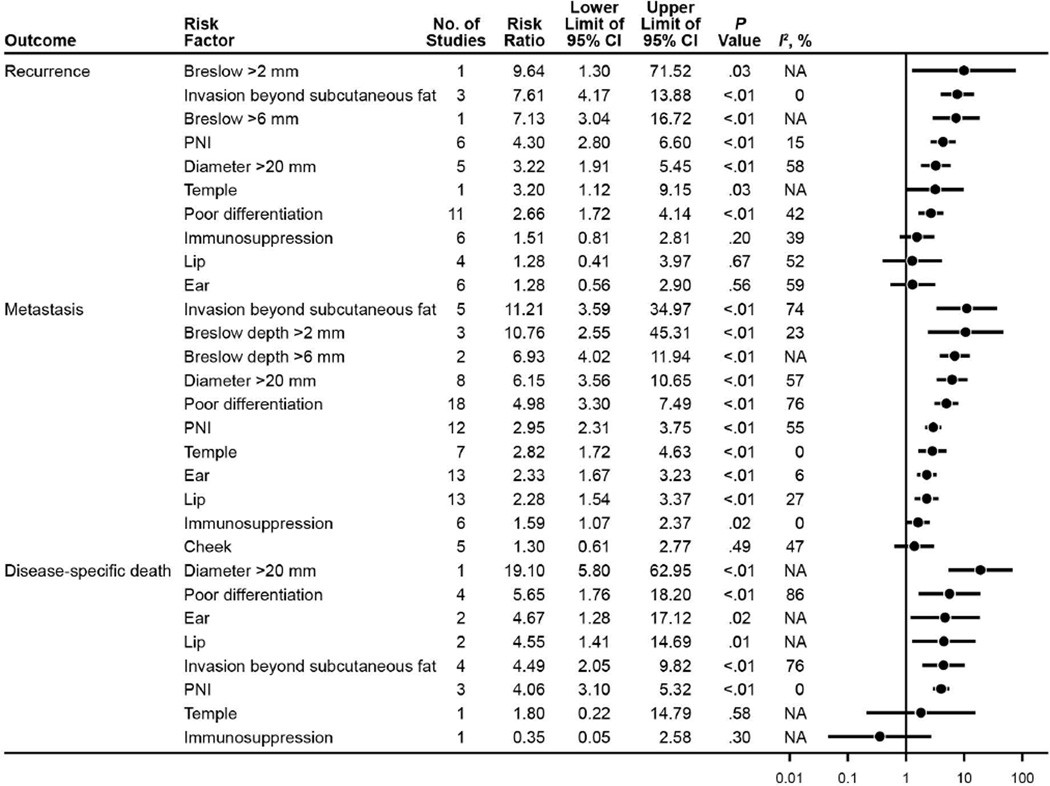
Results: Thirty-six studies (17 248 patients with 23 421 cSCCs) were included. Significant risk factors for recurrence were the following: Breslow thickness exceeding 2 mm (risk ratio [RR], 9.64; 95% CI, 1.30-71.52), invasion beyond subcutaneous fat (RR, 7.61; 95% CI, 4.17-13.88), Breslow thickness exceeding 6 mm (RR, 7.13; 95% CI, 3.04-16.72), perineural invasion (RR, 4.30; 95% CI, 2.80-6.60), diameter exceeding 20 mm (RR, 3.22; 95% CI, 1.91-5.45), location on the temple (RR, 3.20; 95% CI, 1.12-9.15), and poor differentiation (RR, 2.66; 95% CI, 1.72-4.14). Significant risk factors for metastasis were: invasion beyond subcutaneous fat (RR, 11.21; 95% CI, 3.59-34.97), Breslow thickness exceeding 2 mm (RR, 10.76; 95% CI, 2.55-45.31), Breslow thickness exceeding 6 mm (RR, 6.93; 95% CI, 4.02-11.94), diameter exceeding 20 mm (RR, 6.15; 95% CI, 3.56-10.65), poor differentiation (RR, 4.98; 95% CI, 3.30-7.49), perineural invasion (RR, 2.95; 95% CI, 2.31-3.75), immunosuppression (RR, 1.59; 95% CI, 1.07-2.37), and location on the temple (RR, 2.82; 95% CI, 1.72-4.63), ear (RR, 2.33; 95% CI, 1.67-3.23), or lip (RR, 2.28; 95% CI, 1.54-3.37). Significant risk factors for DSD were: diameter exceeding 20 mm (RR, 19.10; 95% CI, 5.80-62.95), poor differentiation (RR, 5.65; 95% CI, 1.76-18.20), location on the ear (RR, 4.67; 95% CI, 1.28-17.12) or lip (RR, 4.55; 95% CI, 1.41-14.69), invasion beyond subcutaneous fat (RR, 4.49; 95% CI, 2.05-9.82), and perineural invasion (RR, 4.06; 95% CI, 3.10-5.32). Evidence quality was considered low to moderate.
Conclusions and relevance: Tumor depth is associated with the highest RR of local recurrence and metastasis of cSCC, and tumor diameter exceeding 20 mm is associated with the highest RR of DSD. Unified, consistent collection and reporting of risk factors in a prospective, multicentered effort are needed to further understand the increasing incidence of cSCC.
Figures
References
-
- Karia PS, Han J, Schmults CD. Cutaneous squamous cell carcinoma: estimated incidence of disease, nodal metastasis, and deaths from disease in the United States, 2012. J Am Acad Dermatol. 2013;68(6):957–966. - PubMed
-
- Rogers HW, Weinstock MA, Harris AR, et al. Incidence estimate of nonmelanoma skin cancer in the United States, 2006. Arch Dermatol. 2010;146(3):283–287. - PubMed
-
- Alam M, Ratner D. Cutaneous squamous-cell carcinoma. N Engl J Med. 2001;344(13):975–983. - PubMed
-
- Brantsch KD, Meisner C, Schonfisch B, et al. Analysis of risk factors determining prognosis of cutaneous squamous-cell carcinoma: a prospective study. Lancet Oncol. 2008;9(8):713–720. - PubMed
-
- Brougham ND, Dennett ER, Cameron R, Tan ST. The incidence of metastasis from cutaneous squamous cell carcinoma and the impact of its risk factors. J Surg Oncol. 2012;106(7):811–815. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
