

Inflammatory bowel disease as a disorder of an imbalance between pro- and anti-inflammatory molecules and deficiency of resolution bioactive lipids
- PMID: 26762544
- PMCID: PMC4712465
- DOI: 10.1186/s12944-015-0165-4
Inflammatory bowel disease as a disorder of an imbalance between pro- and anti-inflammatory molecules and deficiency of resolution bioactive lipids
Abstract
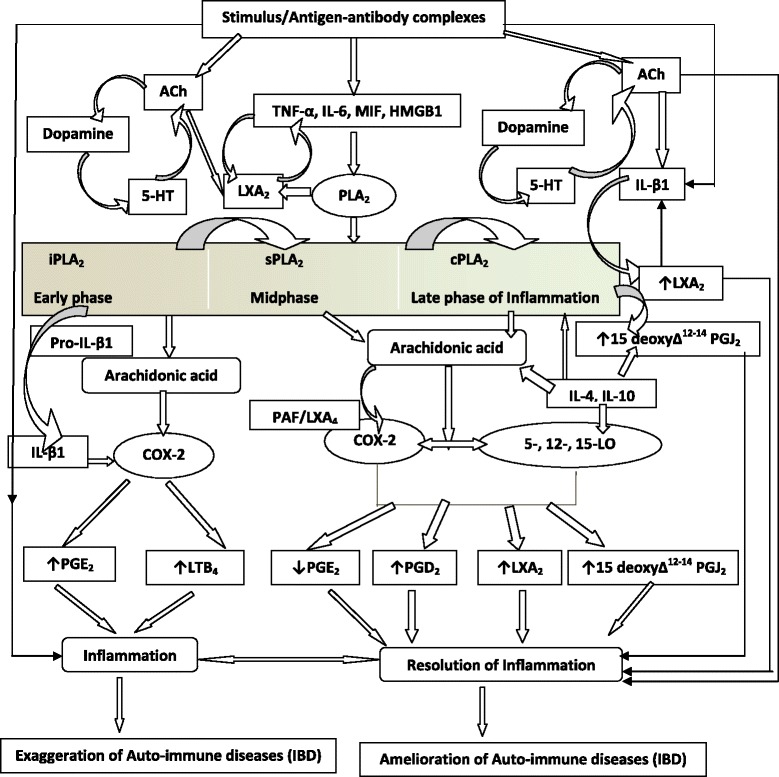
The inflammatory process seen in inflammatory bowel disease (IBD) is due to excess production of pro-inflammatory cytokines interleukin-1 (IL-1), IL-6, tumor necrosis factor-α (TNF-α), interferons (IFNs), macrophage migration inhibitory factor (MIF), HMGB1 (high mobility group B1) and possibly, a reduction in anti-inflammatory cytokines IL-10, IL-4, and transforming growth factor-β (TGF-β). These pro-inflammatory molecules lead to increased production of reactive oxygen species (ROS) including nitric oxide resulting in target tissue damage. I propose that inadequate production of inflammation resolving molecules lipoxins, resolvins, protectins, maresins and nitrolipids that suppress inflammation, ROS production, enhance wound healing and have cytoprotective properties results in inappropriate inflammation, delay in healing/repair process and so target tissue/organ damage continues in IBD. Hence, suggested therapeutic approach could include administration of stable synthetic analogues of lipoxins, resolvins, protectins, maresins and nitrolipids. This implies that measuring urine, stool and plasma levels of lipoxins, resolvins, protectins, maresins and nitrolipids may be used to detect the onset, progression and response to treatment of IBD.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
