

Aggregate and hospital-level impact of national guidelines on diagnostic resource utilization for children with pneumonia at children's hospitals
- PMID: 26762571
- PMCID: PMC5103701
- DOI: 10.1002/jhm.2534
Aggregate and hospital-level impact of national guidelines on diagnostic resource utilization for children with pneumonia at children's hospitals
Abstract
Background: National guidelines for the management of community-acquired pneumonia (CAP) in children were published in 2011. These guidelines discourage most diagnostic testing for outpatients, as well as repeat testing for hospitalized patients who are improving. We sought to evaluate the temporal trends in diagnostic testing associated with guideline implementation among children with CAP.
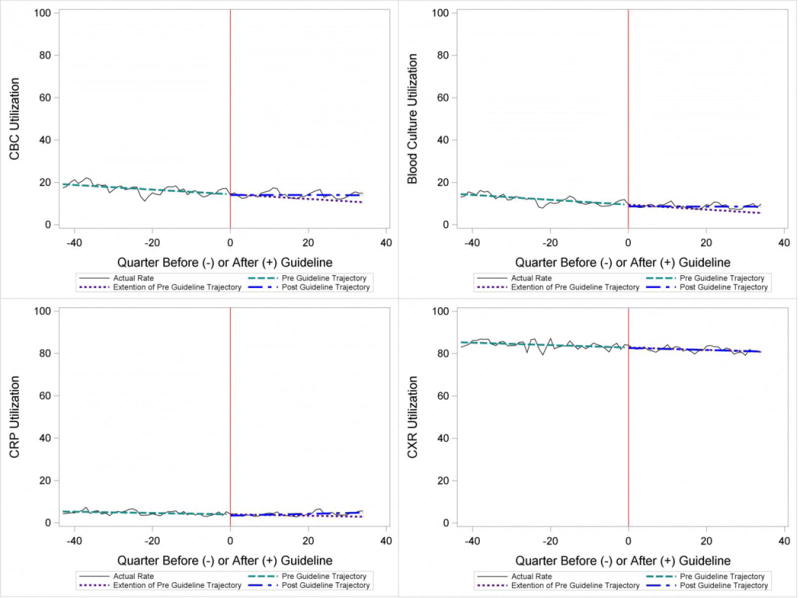
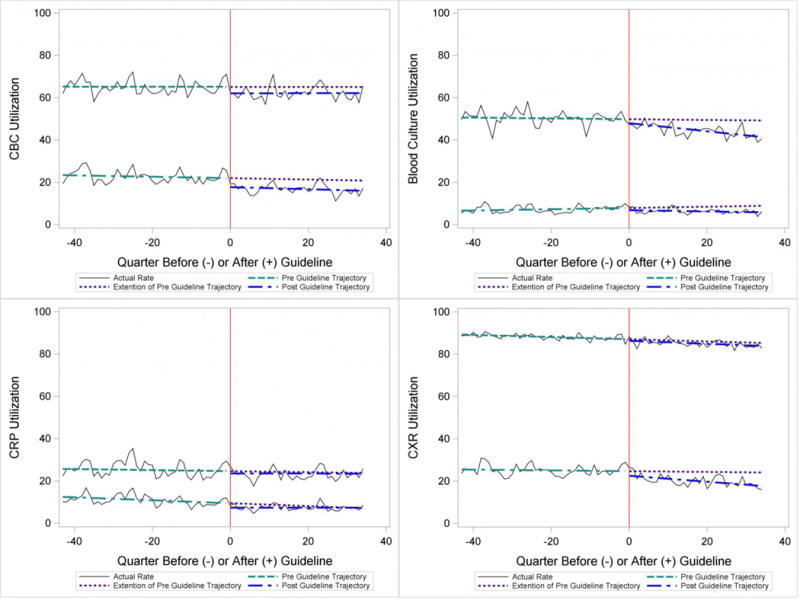
Methods: Children 1 to 18 years old who were discharged with pneumonia after emergency department (ED) evaluation or hospitalization from January 1, 2008 to June 30, 2014 at any of 32 children's hospitals participating in the Pediatric Health Information System were included. We excluded children with complex chronic conditions and those requiring intensive care or who underwent early pleural drainage. We compared use of diagnostic testing (blood culture, complete blood count [CBC], C-reactive protein [CRP], and chest radiography [CXR]) before and after release of the guidelines, and assessed for temporal trends using interrupted time series analysis. We also calculated the cost impact of these changes on diagnostic utilization and evaluated the variability of the guideline's impact across hospitals.
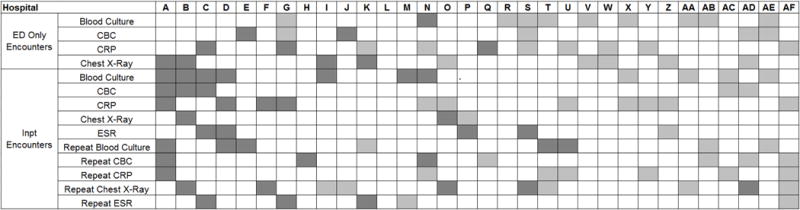
Results: Overall, 220,539 patients were included; 53% were male and the median age was 4 years (interquartile range, 2-7). For patients discharged from the ED with CAP, diagnostic utilization rates for blood culture, CBC, CRP, and CXR were higher after guideline publication compared with expected utilization rates without guidelines. In contrast, initial testing and repeat testing among patients hospitalized with CAP was lower after guideline publication. There were modest reductions in estimated costs associated with these changes. However, wide variability was observed in the impact of the guidelines across hospitals.
Conclusions: Publication of national pneumonia guidelines in 2011 was associated with modest changes in diagnostic testing for children with CAP. However, the changes varied across hospitals, and the financial impact was modest. Local implementation efforts are warranted to ensure widespread guideline adherence. Journal of Hospital Medicine 2016;11:317-323. © 2016 Society of Hospital Medicine.
© 2015 Society of Hospital Medicine.
Conflict of interest statement
Authors have no conflicts of interest
Figures
References
-
- Berwick DM, Hackbarth AD. Eliminating waste in US health care. JAMA. 2012;307(14):1513–6. - PubMed
-
- Quinonez RA, et al. Choosing wisely in pediatric hospital medicine: five opportunities for improved healthcare value. J Hosp Med. 2013;8(9):479–85. - PubMed
-
- Keren R, et al. Prioritization of comparative effectiveness research topics in hospital pediatrics. Arch Pediatr Adolesc Med. 2012;166(12):1155–64. - PubMed
-
- Florin TA, et al. Variation in emergency department diagnostic testing and disposition outcomes in pneumonia. Pediatrics. 2013;132(2):237–44. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
