

Benefit of adjunctive tacrolimus in connective tissue disease-interstitial lung disease
- PMID: 26762710
- PMCID: PMC4760686
- DOI: 10.1016/j.pupt.2015.12.004
Benefit of adjunctive tacrolimus in connective tissue disease-interstitial lung disease
Abstract
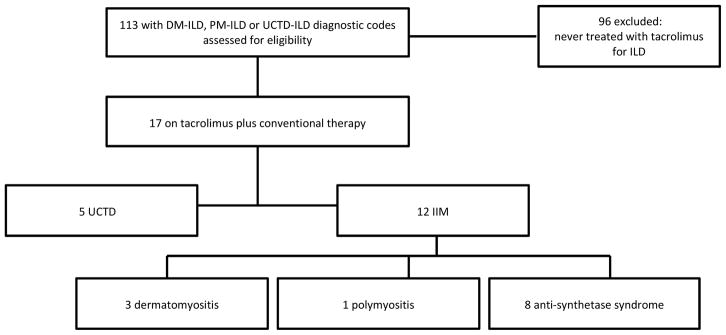
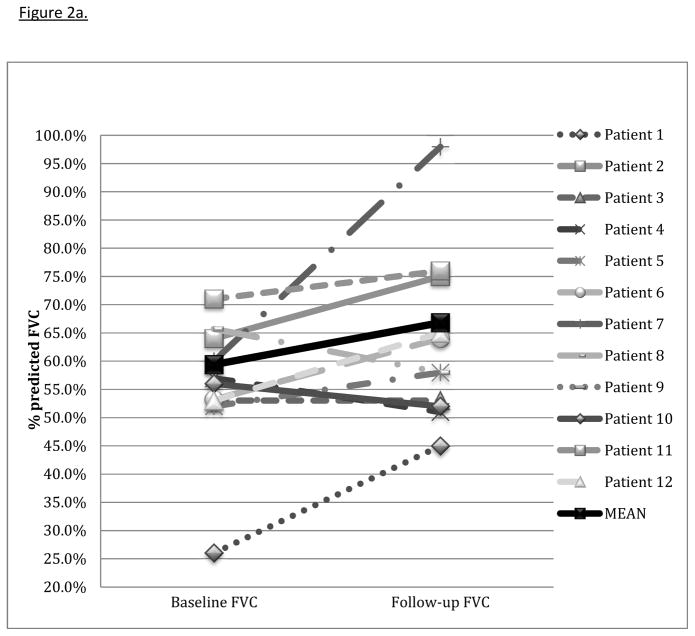
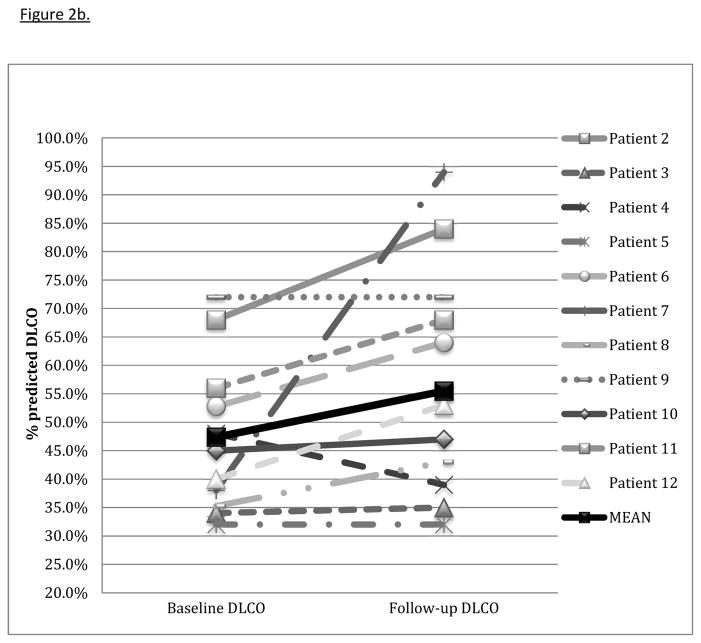
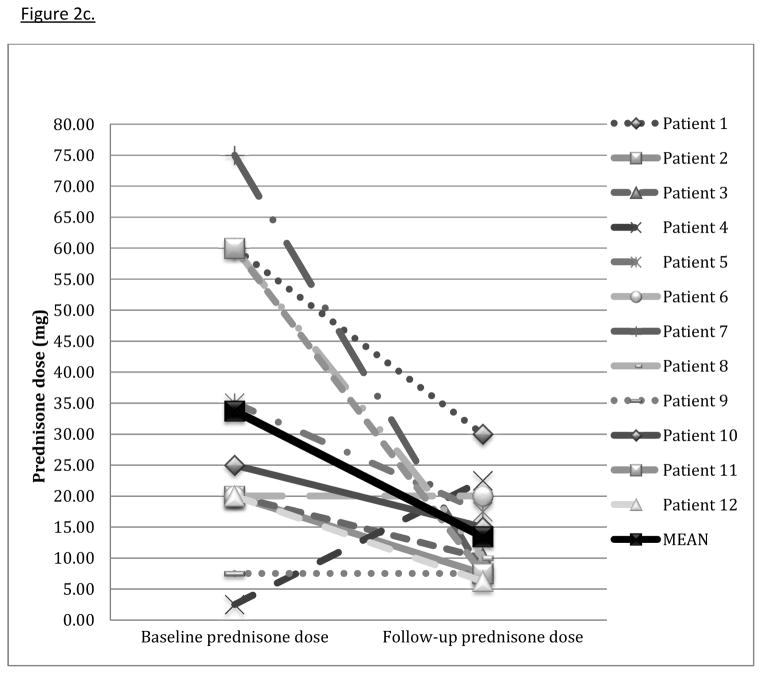
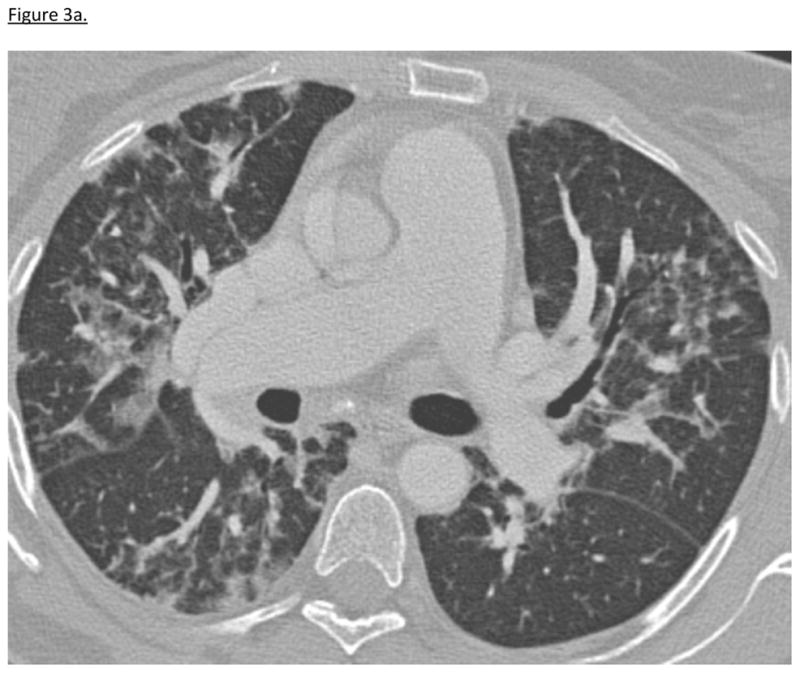
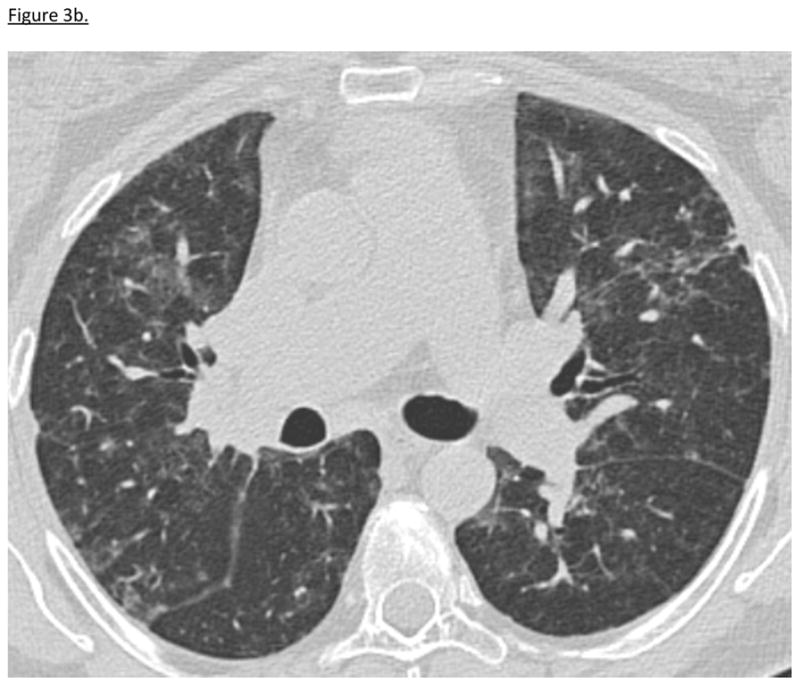
We evaluated the safety and effectiveness of adjunctive tacrolimus therapy with conventional immunosuppression in patients with severe connective tissue disease-related interstitial lung disease (CTD-ILD). We included patients from our interstitial lung disease (ILD) registry with CTD-ILD, in whom tacrolimus was added to corticosteroids and an additional immunosuppressive agent. Demographic data, clinical features, lung function, radiographic images, and pathologic findings were reviewed. Effectiveness was assessed by comparing pulmonary function tests (PFTs) closest to tacrolimus initiation to PFTs approximately 6-12 months later. Corticosteroid dose at these time points was also evaluated. We report adverse events attributed to tacrolimus. Seventeen patients with CTD-ILD were included in adverse event analysis; twelve were included in efficacy analysis. Length of tacrolimus therapy ranged from 6 to 110 months (mean 38.8 months ± 31.4). The mean improvement in percent predicted total lung capacity was 7.5% ± 11.7 (p = 0.02). Forced vital capacity mean improvement was 7.4% ± 12.5 (p = 0.06). The average decrease in corticosteroid dose at follow-up was 20.3 mg ± 25.2 (p = 0.02) with complete discontinuation in six patients. No patients experienced a life-threatening adverse event attributed to tacrolimus. Tacrolimus can be effective and is well tolerated as an adjunctive therapy and allows tapering of corticosteroids.
Keywords: Autoimmune disease; Idiopathic inflammatory myopathies; Immunosuppression; Interstitial lung disease.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Figures
References
-
- Fischer A, du Bois R. Interstitial lung disease in connective tissue disorders. Lancet. 2012;380:689–698. - PubMed
-
- Connors GR, Christopher-Stine L, Oddis CV, Danoff SK. Interstitial lung disease associated with the idiopathic inflammatory myopathies: What progress has been made in the past 35 years? Chest. 2010;138:1464–1474. - PubMed
-
- Marie I, Hachulla E, Cherin P, Dominique S, Hatron PY, Hellot MF, Devulder B, Herson S, Levesque H, Courtois H. Interstitial lung disease in polymyositis and dermatomyositis. Arthritis Care & Research. 2002;47:614–622. - PubMed
-
- Cottin V, Thivolet-Bejui F, Reynaud-Gaubert M, Cadranel J, Delaval P, Ternamian PJ, Cordier JF Groupe d’Etudes et de Recherche sur les Maladies “Orphelines P. Interstitial lung disease in amyopathic dermatomyositis, dermatomyositis and polymyositis. The European respiratory journal : official journal of the European Society for Clinical Respiratory Physiology. 2003;22:245–250. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
