

Prognosis of Myocardial Damage in Sarcoidosis Patients With Preserved Left Ventricular Ejection Fraction: Risk Stratification Using Cardiovascular Magnetic Resonance
- PMID: 26763280
- PMCID: PMC4718184
- DOI: 10.1161/CIRCIMAGING.115.003738
Prognosis of Myocardial Damage in Sarcoidosis Patients With Preserved Left Ventricular Ejection Fraction: Risk Stratification Using Cardiovascular Magnetic Resonance
Abstract
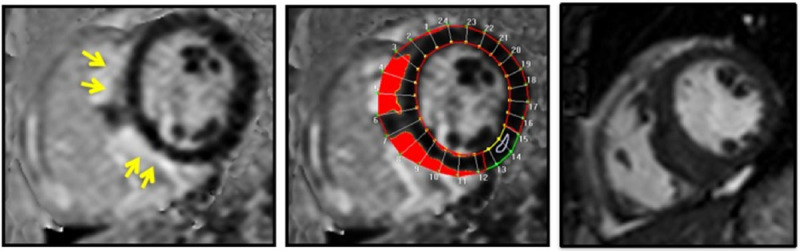
Background: Cardiac sarcoidosis is associated with an increased risk of heart failure and sudden death, but its risk in patients with preserved left ventricular ejection fraction is unknown. Using cardiovascular magnetic resonance in patients with extracardiac sarcoidosis and preserved left ventricular ejection fraction, we sought to (1) determine the prevalence of cardiac sarcoidosis or associated myocardial damage, defined by the presence of late gadolinium enhancement (LGE), (2) quantify their risk of death/ventricular tachycardia (VT), and (3) identify imaging-based covariates that predict who is at greatest risk of death/VT.
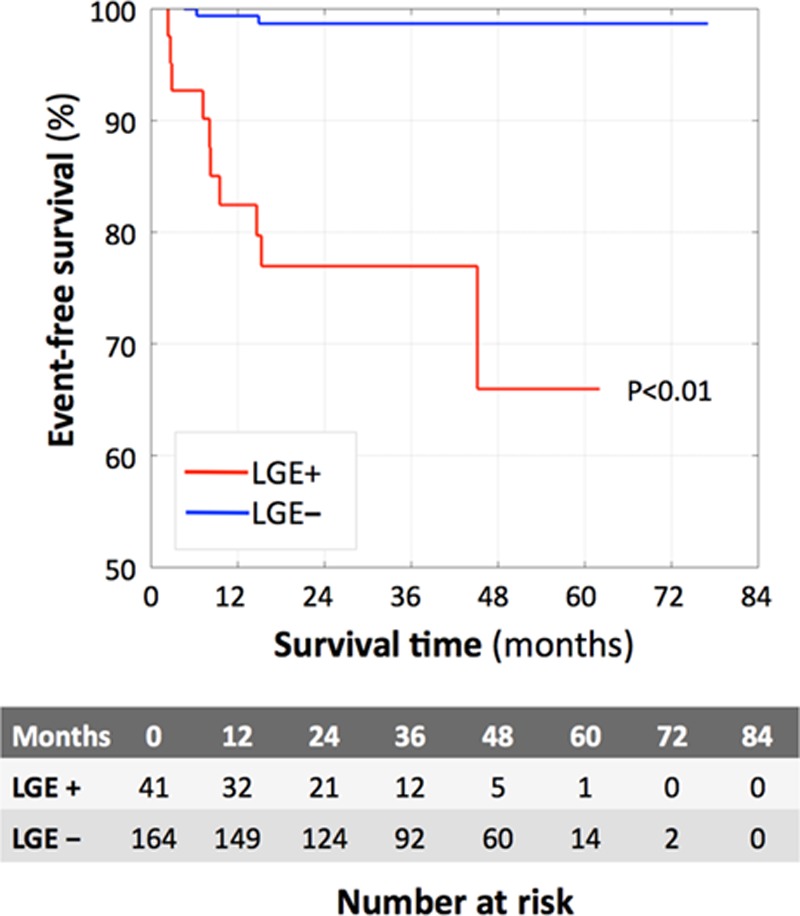
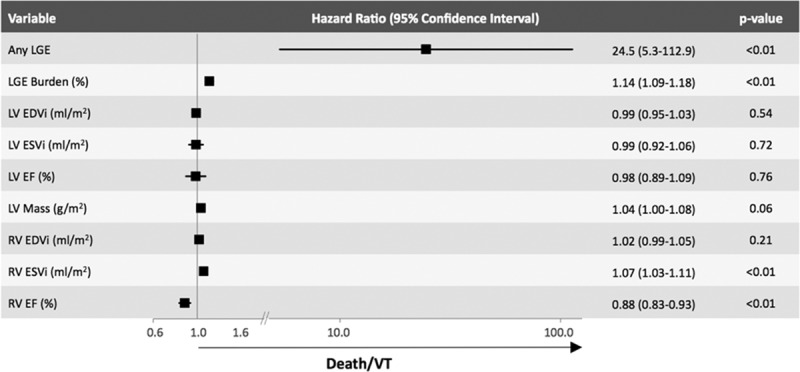
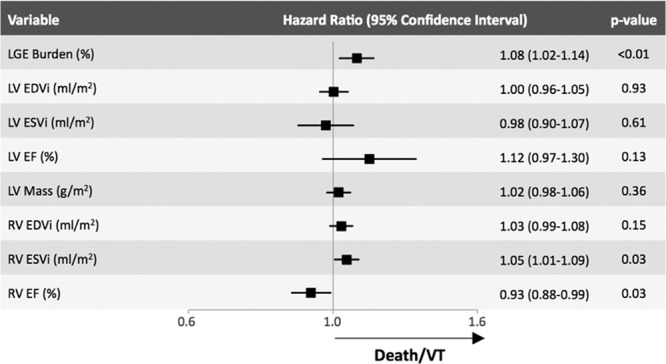
Methods and results: Parameters of left and right ventricular function and LGE burden were measured in 205 patients with left ventricular ejection fraction >50% and extracardiac sarcoidosis who underwent cardiovascular magnetic resonance for LGE evaluation. The association between covariates and death/VT in the entire group and within the LGE+ group was determined using Cox proportional hazard models and time-dependent receiver-operator curves analysis. Forty-one of 205 patients (20%) had LGE; 12 of 205 (6%) died or had VT during follow-up; of these, 10 (83%) were in the LGE+ group. In the LGE+ group (1) the rate of death/VT per year was >20× higher than LGE- (4.9 versus 0.2%, P<0.01); (2) death/VT were associated with a greater burden of LGE (14±11 versus 5±5%, P<0.01) and right ventricular dysfunction (right ventricular EF 45±12 versus 53±28%, P=0.04). LGE burden was the best predictor of death/VT (area under the receiver-operating characteristics curve, 0.80); for every 1% increase of LGE burden, the hazard of death/VT increased by 8%.
Conclusions: Sarcoidosis patients with LGE are at significant risk for death/VT, even with preserved left ventricular ejection fraction. Increased LGE burden and right ventricular dysfunction can identify LGE+ patients at highest risk of death/VT.
Keywords: cardiac arrhythmias; cardiac magnetic resonance; cardiomyopathy; defibrillator; gadolinium; heart failure; sarcoidosis.
© 2016 The Authors.
Figures
Comment in
-
Prognosis of Myocardial Damage in Sarcoidosis Patients With Preserved Left Ventricular Ejection Fraction: Always Look at the Bright Side of Cardiovascular Magnetic Resonance.Circ Cardiovasc Imaging. 2016 Jan;9(1):e004417. doi: 10.1161/CIRCIMAGING.115.004417. Circ Cardiovasc Imaging. 2016. PMID: 26763282 No abstract available.
References
-
- Silverman KJ, Hutchins GM, Bulkley BH. Cardiac sarcoid: a clinicopathologic study of 84 unselected patients with systemic sarcoidosis. Circulation. 1978;58:1204–1211. - PubMed
-
- Banba K, Kusano KF, Nakamura K, Morita H, Ogawa A, Ohtsuka F, Ogo KO, Nishii N, Watanabe A, Nagase S, Sakuragi S, Ohe T. Relationship between arrhythmogenesis and disease activity in cardiac sarcoidosis. Heart Rhythm. 2007;4:1292–1299. doi: 10.1016/j.hrthm.2007.06.006. - PubMed
-
- Viles-Gonzalez JF, Pastori L, Fischer A, Wisnivesky JP, Goldman MG, Mehta D. Supraventricular arrhythmias in patients with cardiac sarcoidosis prevalence, predictors, and clinical implications. Chest. 2013;143:1085–1090. - PubMed
-
- Cain MA, Metzl MD, Patel AR, Addetia K, Spencer KT, Sweiss NJ, Beshai JF. Cardiac sarcoidosis detected by late gadolinium enhancement and prevalence of atrial arrhythmias. Am J Cardiol. 2014;113:1556–1560. doi: 10.1016/j.amjcard.2014.01.434. - PubMed
-
- Epstein AE, DiMarco JP, Ellenbogen KA, Estes NA, III, Freedman RA, Gettes LS, Gillinov AM, Gregoratos G, Hammill SC, Hayes DL, Hlatky MA, Newby LK, Page RL, Schoenfeld MH, Silka MJ, Stevenson LW, Sweeney MO, Smith SC, Jr, Jacobs AK, Adams CD, Anderson JL, Buller CE, Creager MA, Ettinger SM, Faxon DP, Halperin JL, Hiratzka LF, Hunt SA, Krumholz HM, Kushner FG, Lytle BW, Nishimura RA, Ornato JP, Page RL, Riegel B, Tarkington LG, Yancy CW American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices); American Association for Thoracic Surgery; Society of Thoracic Surgeons. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices) developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;51:e1–62. doi: 10.1016/j.jacc.2008.02.032. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
