

The pertussis enigma: reconciling epidemiology, immunology and evolution
- PMID: 26763701
- PMCID: PMC4721090
- DOI: 10.1098/rspb.2015.2309
The pertussis enigma: reconciling epidemiology, immunology and evolution
Abstract
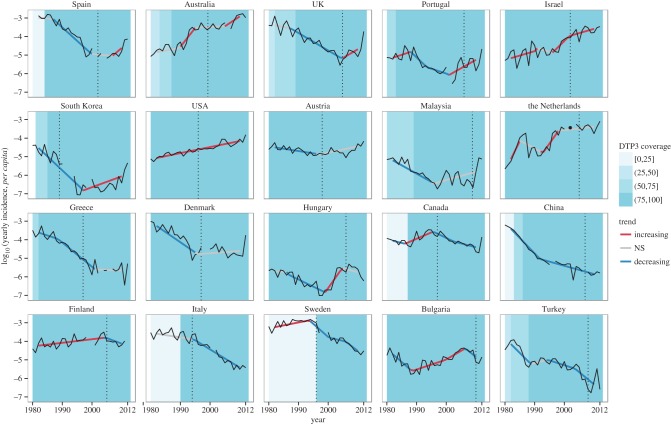
Pertussis, a highly contagious respiratory infection, remains a public health priority despite the availability of vaccines for 70 years. Still a leading cause of mortality in developing countries, pertussis has re-emerged in several developed countries with high vaccination coverage. Resurgence of pertussis in these countries has routinely been attributed to increased awareness of the disease, imperfect vaccinal protection or high infection rates in adults. In this review, we first present 1980-2012 incidence data from 63 countries and show that pertussis resurgence is not universal. We further argue that the large geographical variation in trends probably precludes a simple explanation, such as the transition from whole-cell to acellular pertussis vaccines. Reviewing available evidence, we then propose that prevailing views on pertussis epidemiology are inconsistent with both historical and contemporary data. Indeed, we summarize epidemiological evidence showing that natural infection and vaccination both appear to provide long-term protection against transmission and disease, so that previously infected or vaccinated adults contribute little to overall transmission at a population level. Finally, we identify several promising avenues that may lead to a consistent explanation of global pertussis epidemiology and to more effective control strategies.
Keywords: infection-derived immunity; pertussis; pertussis epidemiology; pertussis resurgence; pertussis vaccines; vaccine-derived immunity.
© 2016 The Author(s).
Figures
References
-
- Edwards KM, Decker MD. 2013. Pertussis vaccines. In Vaccines (eds SA Plotkin, WA Orenstein, PA Offit), pp. 447–492. Philadelphia, PA: Elsevier Saunders.
-
- World Health Organization 2010. Pertussis vaccines: WHO position paper. Wkly Epidemiol. Rec. 85, 385–400. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous