

Coronary plaque quantification and fractional flow reserve by coronary computed tomography angiography identify ischaemia-causing lesions
- PMID: 26763790
- PMCID: PMC4830909
- DOI: 10.1093/eurheartj/ehv690
Coronary plaque quantification and fractional flow reserve by coronary computed tomography angiography identify ischaemia-causing lesions
Abstract
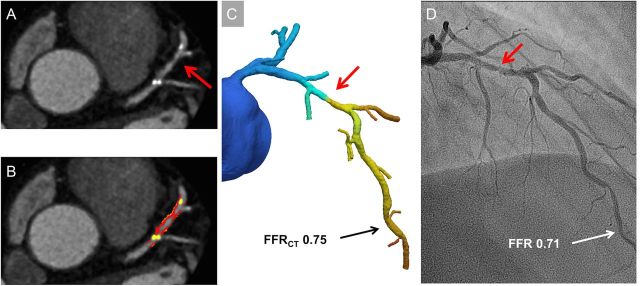
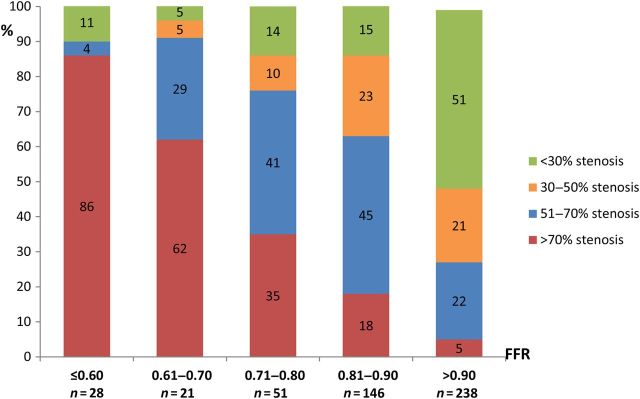
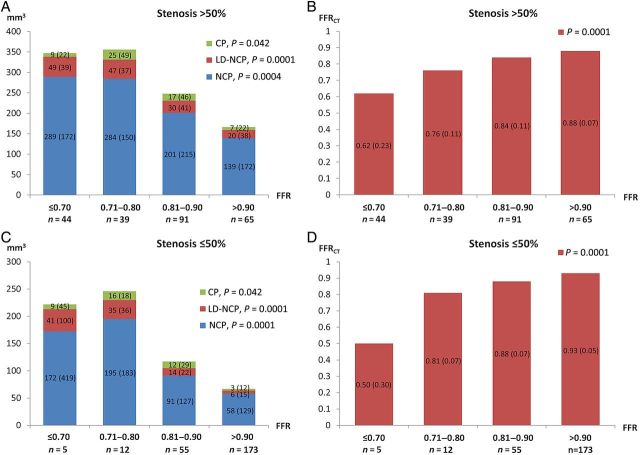
Aims: Coronary plaque characteristics are associated with ischaemia. Differences in plaque volumes and composition may explain the discordance between coronary stenosis severity and ischaemia. We evaluated the association between coronary stenosis severity, plaque characteristics, coronary computed tomography angiography (CTA)-derived fractional flow reserve (FFRCT), and lesion-specific ischaemia identified by FFR in a substudy of the NXT trial (Analysis of Coronary Blood Flow Using CT Angiography: Next Steps).
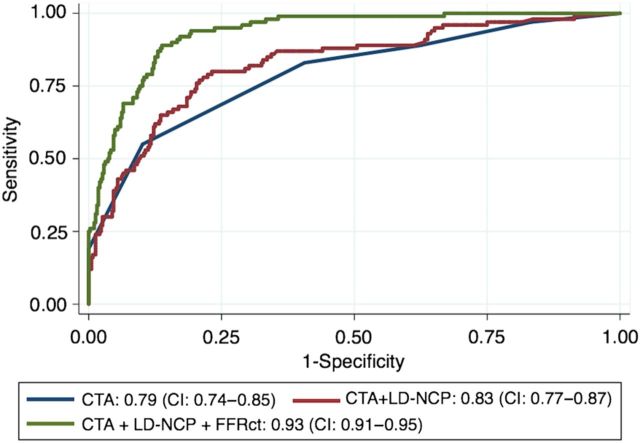
Methods and results: Coronary CTA stenosis, plaque volumes, FFRCT, and FFR were assessed in 484 vessels from 254 patients. Stenosis >50% was considered obstructive. Plaque volumes (non-calcified plaque [NCP], low-density NCP [LD-NCP], and calcified plaque [CP]) were quantified using semi-automated software. Optimal thresholds of quantitative plaque variables were defined by area under the receiver-operating characteristics curve (AUC) analysis. Ischaemia was defined by FFR or FFRCT ≤0.80. Plaque volumes were inversely related to FFR irrespective of stenosis severity. Relative risk (95% confidence interval) for prediction of ischaemia for stenosis >50%, NCP ≥185 mm(3), LD-NCP ≥30 mm(3), CP ≥9 mm(3), and FFRCT ≤0.80 were 5.0 (3.0-8.3), 3.7 (2.4-5.6), 4.6 (2.9-7.4), 1.4 (1.0-2.0), and 13.6 (8.4-21.9), respectively. Low-density NCP predicted ischaemia independent of other plaque characteristics. Low-density NCP and FFRCT yielded diagnostic improvement over stenosis assessment with AUCs increasing from 0.71 by stenosis >50% to 0.79 and 0.90 when adding LD-NCP ≥30 mm(3) and LD-NCP ≥30 mm(3) + FFRCT ≤0.80, respectively.
Conclusion: Stenosis severity, plaque characteristics, and FFRCT predict lesion-specific ischaemia. Plaque assessment and FFRCT provide improved discrimination of ischaemia compared with stenosis assessment alone.
Keywords: Computational fluid dynamics; Computed tomography angiography; Coronary plaque; Fractional flow reserve; Ischaemia.
© The Author 2016. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Anatomy and physiology in ischaemic heart disease: a second honeymoon?Eur Heart J. 2016 Apr 14;37(15):1228-31. doi: 10.1093/eurheartj/ehv748. Epub 2016 Jan 18. Eur Heart J. 2016. PMID: 26787439 No abstract available.
Similar articles
-
Non-invasive fractional flow reserve in vessels without severe obstructive stenosis is associated with coronary plaque burden.J Cardiovasc Comput Tomogr. 2018 Sep-Oct;12(5):379-384. doi: 10.1016/j.jcct.2018.05.003. Epub 2018 May 7. J Cardiovasc Comput Tomogr. 2018. PMID: 29784622
-
Integrated prediction of lesion-specific ischaemia from quantitative coronary CT angiography using machine learning: a multicentre study.Eur Radiol. 2018 Jun;28(6):2655-2664. doi: 10.1007/s00330-017-5223-z. Epub 2018 Jan 19. Eur Radiol. 2018. PMID: 29352380 Free PMC article. Clinical Trial.
-
CT-based total vessel plaque analyses improves prediction of hemodynamic significance lesions as assessed by fractional flow reserve in patients with stable angina pectoris.J Cardiovasc Comput Tomogr. 2018 Jul-Aug;12(4):344-349. doi: 10.1016/j.jcct.2018.04.008. Epub 2018 May 8. J Cardiovasc Comput Tomogr. 2018. PMID: 29866619 Clinical Trial.
-
Beyond Stenosis With Fractional Flow Reserve Via Computed Tomography and Advanced Plaque Analyses for the Diagnosis of Lesion-Specific Ischemia.Can J Cardiol. 2016 Nov;32(11):1315.e1-1315.e9. doi: 10.1016/j.cjca.2016.01.023. Epub 2016 Jan 29. Can J Cardiol. 2016. PMID: 27032888 Review.
-
Computed tomography angiography-derived fractional flow reserve (CT-FFR) for the detection of myocardial ischemia with invasive fractional flow reserve as reference: systematic review and meta-analysis.Eur Radiol. 2020 Feb;30(2):712-725. doi: 10.1007/s00330-019-06470-8. Epub 2019 Nov 6. Eur Radiol. 2020. PMID: 31696294
Cited by
-
Predicting Chronic Myocardial Ischemia Using CCTA-Based Radiomics Machine Learning Nomogram.J Nucl Cardiol. 2022 Feb;29(1):262-274. doi: 10.1007/s12350-020-02204-2. Epub 2020 Jun 18. J Nucl Cardiol. 2022. PMID: 32557238 Clinical Trial.
-
Machine Learning From Quantitative Coronary Computed Tomography Angiography Predicts Fractional Flow Reserve-Defined Ischemia and Impaired Myocardial Blood Flow.Circ Cardiovasc Imaging. 2022 Oct;15(10):e014369. doi: 10.1161/CIRCIMAGING.122.014369. Epub 2022 Oct 13. Circ Cardiovasc Imaging. 2022. PMID: 36252116 Free PMC article. Clinical Trial.
-
Catheter-based functional metrics of the coronary circulation.J Nucl Cardiol. 2017 Aug;24(4):1178-1189. doi: 10.1007/s12350-016-0652-7. Epub 2016 Sep 7. J Nucl Cardiol. 2017. PMID: 27604111
-
Artificial Intelligence in Cardiovascular Atherosclerosis Imaging.J Pers Med. 2022 Mar 8;12(3):420. doi: 10.3390/jpm12030420. J Pers Med. 2022. PMID: 35330420 Free PMC article. Review.
-
Comparison of mineral oil and non-mineral oil placebo on coronary plaque progression by coronary computed tomography angiography.Cardiovasc Res. 2020 Mar 1;116(3):479-482. doi: 10.1093/cvr/cvz329. Cardiovasc Res. 2020. PMID: 31825484 Free PMC article. No abstract available.
References
-
- Meijboom WB, Van Mieghem CA, van Pelt N, Weustink A, Pugliese F, Mollet NR, Boersma E, Regar E, van Geuns RJ, de Jaegere PJ, Serruys PW, Krestin GP, de Feyter PJ. Comprehensive assessment of coronary artery stenoses: computed tomography coronary angiography versus conventional coronary angiography and correlation with fractional flow reserve in patients with stable angina. J Am Coll Cardiol 2008;52:636–643. - PubMed
-
- Shaw LJ, Berman DS, Maron DJ, Mancini GB, Hayes SW, Hartigan PM, Weintraub WS, O'Rourke RA, Dada M, Spertus JA, Chaitman BR, Friedman J, Slomka P, Heller GV, Germano G, Gosselin G, Berger P, Kostuk WJ, Schwartz RG, Knudtson M, Veledar E, Bates ER, McCallister B, Teo KK, Boden WE, COURAGE Investigators. Optimal medical therapy with or without percutaneous coronary intervention to reduce ischemic burden: results from the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial nuclear substudy. Circulation 2008;117:1283–1291. - PubMed
-
- Curzen N, Rana O, Nicholas Z, Golledge P, Zaman A, Oldroyd K, Hanratty C, Banning A, Wheatcroft S, Hobson A, Chitkara K, Hildick-Smith D, McKenzie D, Calver A, Dimitrov BD, Corbett S. Does routine pressure wire assessment influence management strategy at coronary angiography for diagnosis of chest pain? The RIPCORD study. Circ Cardiovasc Interv 2014;7:248–255. - PubMed
-
- Schuijf JD, Wijns W, Jukema JW, Atsma DE, de Roos A, Lamb HJ, Stokkel MP, Dibbets-Schneider P, Decramer I, De Bondt P, van der Wall EE, Vanhoenacker PK, Bax JJ. Relationship between noninvasive coronary angiography with multi-slice computed tomography and myocardial perfusion imaging. J Am Coll Cardiol 2006;48:2508–2514. - PubMed
-
- Park HB, Heo R, O Hartaigh B, Cho I, Gransar H, Nakazato R, Leipsic J, Mancini GB, Koo BK, Otake H, Budoff MJ, Berman DS, Erglis A, Chang HJ, Min JK. Atherosclerotic plaque characteristics by CT angiography identify coronary lesions that cause ischemia: a direct comparison to fractional flow reserve. JACC Cardiovasc Imaging 2015;8:1–10. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
