

Hypochloraemia is strongly and independently associated with mortality in patients with chronic heart failure
- PMID: 26763893
- PMCID: PMC5471359
- DOI: 10.1002/ejhf.477
Hypochloraemia is strongly and independently associated with mortality in patients with chronic heart failure
Abstract
Aims: Hyponatraemia is strongly associated with adverse outcomes in heart failure. However, accumulating evidence suggests that chloride may play an important role in renal salt sensing and regulation of neurohormonal and sodium-conserving pathways. Our objective was to determine the prognostic importance of hypochloraemia in patients with heart failure.
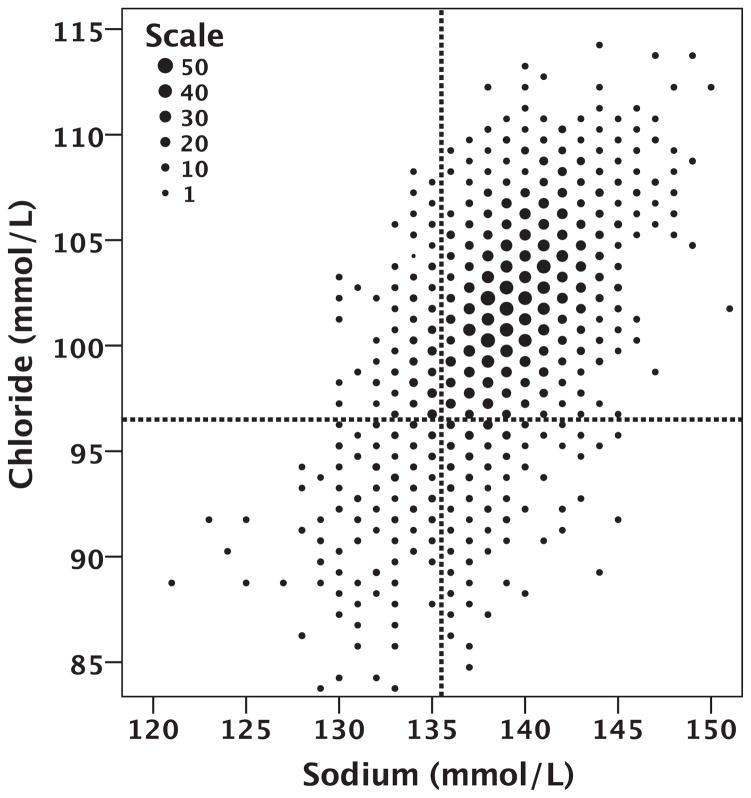
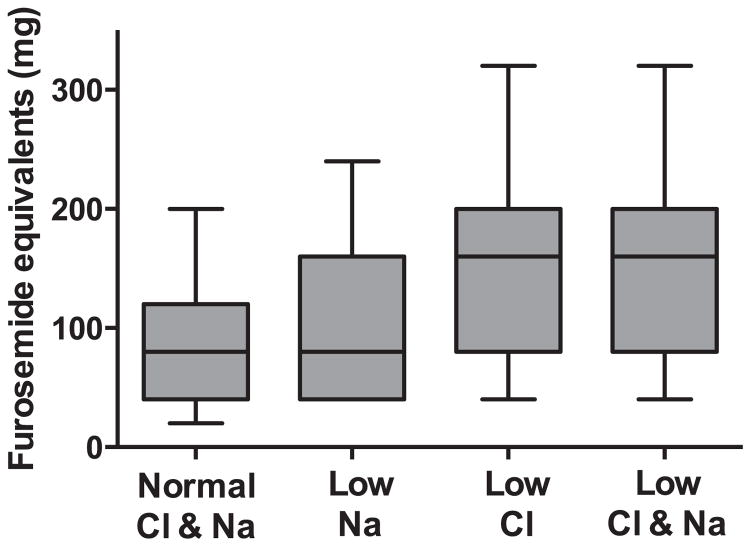
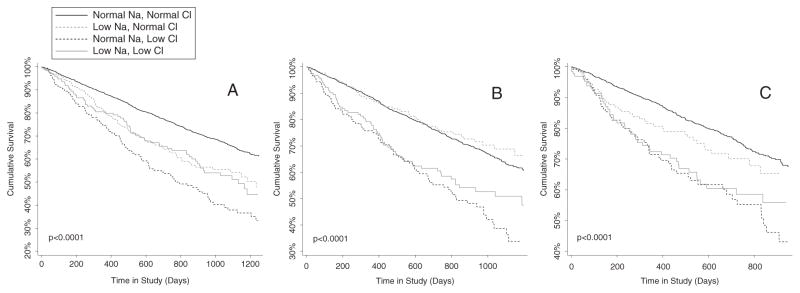
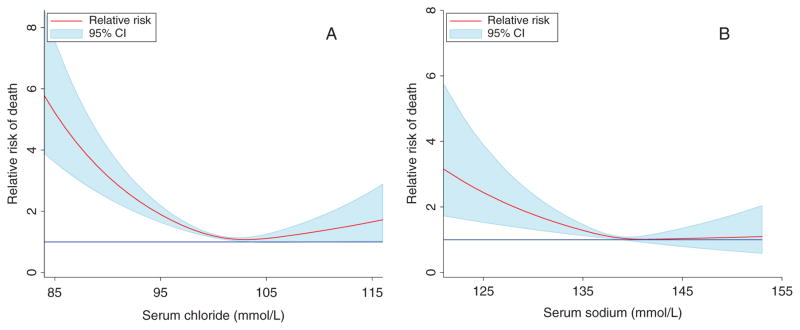
Methods and results: Patients in the BEST trial with baseline serum chloride values were evaluated (n = 2699). Hypochloraemia was defined as a serum chloride ≤96 mmol/L and hyponatraemia as serum sodium ≤135 mmol/L. Hypochloraemia was present in 13.0% and hyponatraemia in 13.7% of the population. Chloride and sodium were only modestly correlated (r = 0.53), resulting in only 48.7% of hypochloraemic patients having concurrent hyponatraemia. Both hyponatraemia and hypochloraemia identified a population with greater disease severity; however, renal function tended to be worse and loop diuretic doses higher with hypochloraemia. In univariate analysis, lower serum sodium or serum chloride as continuous parameters were each strongly associated with mortality (P < 0.001). However, when both parameters were included in the same model, serum chloride remained strongly associated with mortality [hazard ratio (HR) 1.3 per standard deviation decrease, 95% confidence interval (CI) 1.18-1.42, P < 0.001], whereas sodium was not (HR 0.97 per standard deviation decrease, 95% CI 0.89-1.06, P = 0.52).
Conclusion: Serum chloride is strongly and independently associated with worsened survival in patients with chronic heart failure and accounted for the majority of the risk otherwise attributable to hyponatraemia. Given the critical role of chloride in a number of regulatory pathways central to heart failure pathophysiology, additional research is warranted in this area.
Keywords: Heart failure; Hypochloraemia; Hyponatraemia; Mortality; Serum chloride; Serum sodium.
© 2016 The Authors European Journal of Heart Failure © 2016 European Society of Cardiology.
Conflict of interest statement
Figures
Comment in
-
Serum chloride in heart failure: a salty prognosis.Eur J Heart Fail. 2016 Jun;18(6):669-71. doi: 10.1002/ejhf.546. Epub 2016 Apr 27. Eur J Heart Fail. 2016. PMID: 27121684 No abstract available.
References
-
- Hauptman PJ. Clinical challenge of hyponatremia in heart failure. J Hosp Med. 2012;7(Suppl 4):S6–S10. - PubMed
-
- Rusinaru D, Tribouilloy C, Berry C, Richards AM, Whalley GA, Earle N, Poppe KK, Guazzi M, Macin SM, Komajda M, Doughty RN. Relationship of serum sodium concentration to mortality in a wide spectrum of heart failure patients with preserved and with reduced ejection fraction: an individual patient data meta-analysis: Meta-Analysis Global Group in Chronic heart failure (MAGGIC) Eur J Heart Fail. 2012;14:1139–1146. - PubMed
-
- Goldsmith SR. Current treatments and novel pharmacologic treatments for hyponatremia in congestive heart failure. Am J Cardiol. 2005;95:14B–23B. - PubMed
-
- De Luca L, Klein L, Udelson JE, Orlandi C, Sardella G, Fedele F, Gheorghiade M. Hyponatremia in patients with heart failure. Am J Cardiol. 2005;96:19 L–23 L. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
