

The Impact of Cognitive Stressors in the Emergency Department on Physician Implicit Racial Bias
- PMID: 26763939
- PMCID: PMC5020698
- DOI: 10.1111/acem.12901
The Impact of Cognitive Stressors in the Emergency Department on Physician Implicit Racial Bias
Abstract
Objectives: The emergency department (ED) is characterized by stressors (e.g., fatigue, stress, time pressure, and complex decision-making) that can pose challenges to delivering high-quality, equitable care. Although it has been suggested that characteristics of the ED may exacerbate reliance on cognitive heuristics, no research has directly investigated whether stressors in the ED impact physician racial bias, a common heuristic. We seek to determine if physicians have different levels of implicit racial bias post-ED shift versus preshift and to examine associations between demographics and cognitive stressors with bias.
Methods: This repeated-measures study of resident physicians in a pediatric ED used electronic pre- and postshift assessments of implicit racial bias, demographics, and cognitive stressors. Implicit bias was measured using the Race Implicit Association Test (IAT). Linear regression models compared differences in IAT scores pre- to postshift and determined associations between participant demographics and cognitive stressors with postshift IAT and pre- to postshift difference scores.
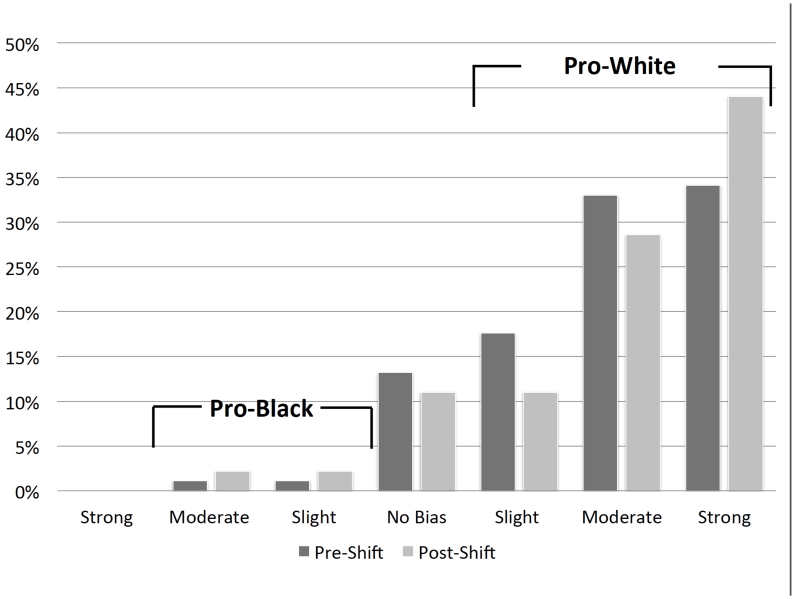
Results: Participants (n = 91) displayed moderate prowhite/antiblack bias on preshift (mean ± SD = 0.50 ± 0.34, d = 1.48) and postshift (mean ± SD = 0.55 ± 0.39, d = 1.40) IAT scores. Overall, IAT scores did not differ preshift to postshift (mean increase = 0.05, 95% CI = -0.02 to 0.14, d = 0.13). Subanalyses revealed increased pre- to postshift bias among participants working when the ED was more overcrowded (mean increase = 0.09, 95% CI = 0.01 to 0.17, d = 0.24) and among those caring for >10 patients (mean increase = 0.17, 95% CI = 0.05 to 0.27, d = 0.47). Residents' demographics (including specialty), fatigue, busyness, stressfulness, and number of shifts were not associated with postshift IAT or difference scores. In multivariable models, ED overcrowding was associated with greater postshift bias (coefficient = 0.11 per 1 unit of NEDOCS score, SE = 0.05, 95% CI = 0.00 to 0.21).
Conclusions: While resident implicit bias remained stable overall preshift to postshift, cognitive stressors (overcrowding and patient load) were associated with increased implicit bias. Physicians in the ED should be aware of how cognitive stressors may exacerbate implicit racial bias.
© 2016 by the Society for Academic Emergency Medicine.
Figures
References
-
- Kovacs G, Croskerry P. Clinical decision making: an emergency medicine perspective. Acad Emerg Med. 1999;6(9):947–52. - PubMed
-
- Croskerry P, Sinclair D. Emergency medicine: a practice prone to error? CJEM. 2001;3(4):271–6. - PubMed
-
- Krug SE, Frush K. Patient safety in the pediatric emergency care setting. Pediatrics. 2007;120(6):1367–75. - PubMed
-
- Coiera EW, Jayasuriya RA, Hardy J, Bannan A, Thorpe ME. Communication loads on clinical staff in the emergency department. Med J Aust. 2002;176(9):415–8. - PubMed
-
- Laxmisan A, Hakimzada F, Sayan OR, Green RA, Zhang J, Patel VL. The multitasking clinician: decision-making and cognitive demand during and after team handoffs in emergency care. Int J Med Inform. 2007;76(11-12):801–11. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
