

Optimizing the G8 Screening Tool for Older Patients With Cancer: Diagnostic Performance and Validation of a Six-Item Version
- PMID: 26764250
- PMCID: PMC4746091
- DOI: 10.1634/theoncologist.2015-0326
Optimizing the G8 Screening Tool for Older Patients With Cancer: Diagnostic Performance and Validation of a Six-Item Version
Abstract
Background: A multidimensional geriatric assessment (GA) is recommended in older cancer patients to inventory health problems and tailor treatment decisions accordingly but requires considerable time and human resources. The G8 is among the most sensitive screening tools for selecting patients warranting a full GA but has limited specificity. We sought to develop and validate an optimized version of the G8.
Patients and methods: We used a prospective cohort of cancer patients aged ≥ 70 years referred to geriatricians for GA (2007-2012: n = 729 [training set]; 2012-2014: n = 414 [validation set]). Abnormal GA was defined as at least one impaired domain across seven validated tests. Multiple correspondence analysis, multivariate logistic regression, and bootstrapped internal validation were performed sequentially.
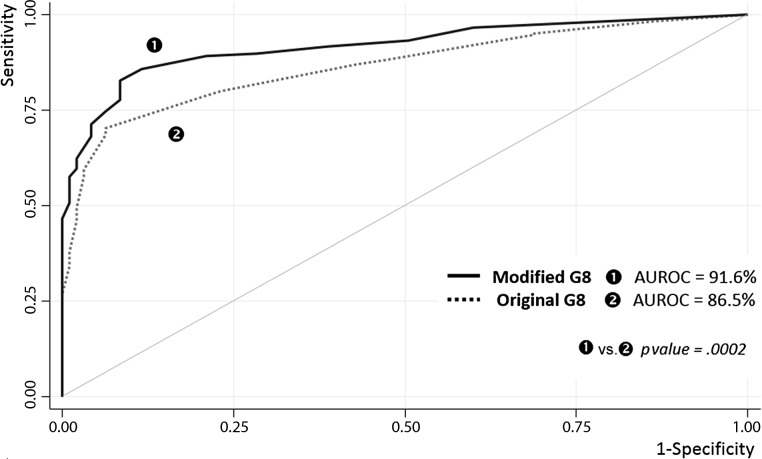
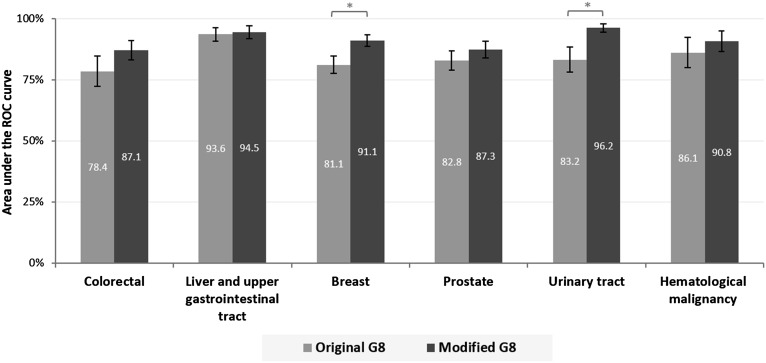
Results: The final model included six independent predictors for abnormal GA: weight loss, cognition/mood, performance status, self-rated health status, polypharmacy (≥ 6 medications per day), and history of heart failure/coronary heart disease. For the original G8, sensitivity was 87.2% (95% confidence interval, 84.3-89.7), specificity 57.7% (47.3-67.7), and area under the receiver-operating characteristic curve (AUROC) 86.5% (83.5-89.6). The modified G8 had corresponding values of 89.2% (86.5-91.5), 79.0% (69.4-86.6), and 91.6% (89.3; 93.9), with higher AUROC values for all tumor sites and stable properties on the validation set.
Conclusion: A modified G8 screening tool exhibited better diagnostic performance with greater uniformity across cancer sites and required only six items. If these features are confirmed in other settings, the modified tool may facilitate selection for a full GA in older patients with cancer.
Implications for practice: Several screening tools have been developed to identify older patients with cancer likely to benefit from a complete geriatric assessment, but none combines appropriate sensitivity and specificity. Based on a large prospective cohort study, an optimized G8 tool was developed, combining a systematic statistical approach with expert judgment to ensure optimal discriminative power and clinical relevance. The improved screening tool achieves high sensitivity, high specificity, better homogeneity across cancer types, and greater parsimony with only six items needed, facilitating selection for a full geriatric assessment.
Keywords: Cancer; Frailty; Geriatric assessment; Sensitivity and specificity.
©AlphaMed Press.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures
References
-
- Howlader N, Noone A, Krapcho M et al. SEER Cancer Statistics Review, 1975–2011. Bethesda, MD: National Cancer Institute. Available at http://seer.cancer.gov/archive/csr/1975_2011/. Accessed August 1, 2015.
-
- Extermann M, Aapro M, Bernabei R, et al. Use of comprehensive geriatric assessment in older cancer patients: Recommendations from the task force on CGA of the International Society of Geriatric Oncology (SIOG) Crit Rev Oncol Hematol. 2005;55:241–252. - PubMed
-
- Rubenstein LZ, Stuck AE, Siu AL, et al. Impacts of geriatric evaluation and management programs on defined outcomes: Overview of the evidence. J Am Geriatr Soc. 1991;39:8S–18S. - PubMed
-
- Puts MT, Santos B, Hardt J, et al. An update on a systematic review of the use of geriatric assessment for older adults in oncology. Ann Oncol. 2014;25:307–315. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
