

Predictive Values of N-Terminal Pro-B-Type Natriuretic Peptide and Cardiac Troponin I for Myocardial Fibrosis in Hypertrophic Obstructive Cardiomyopathy
- PMID: 26765106
- PMCID: PMC4713160
- DOI: 10.1371/journal.pone.0146572
Predictive Values of N-Terminal Pro-B-Type Natriuretic Peptide and Cardiac Troponin I for Myocardial Fibrosis in Hypertrophic Obstructive Cardiomyopathy
Abstract
Background: Both high-sensitivity cardiac troponin T and B-type natriuretic peptide are useful in detecting myocardial fibrosis, as determined by late gadolinium enhancement (LGE) cardiovascular magnetic resonance (CMR), in patients with non-obstructive hypertrophic cardiomyopathy. However, their values to predict myocardial fibrosis in hypertrophic obstructive cardiomyopathy (HOCM) remain unclear. We investigated the role of N-Terminal Pro-B-Type Natriuretic Peptide (NT-proBNP) and cardiac troponin I (cTnI) to identify LGE-CMR in patients with HOCM.
Methods: Peripheral concentrations of NT-proBNP and cTnI were determined in patients with HOCM (n = 163; age = 47.2 ± 10.8 years; 38.7% females). Contrast-enhanced CMR was performed to identify and quantify myocardial fibrosis.
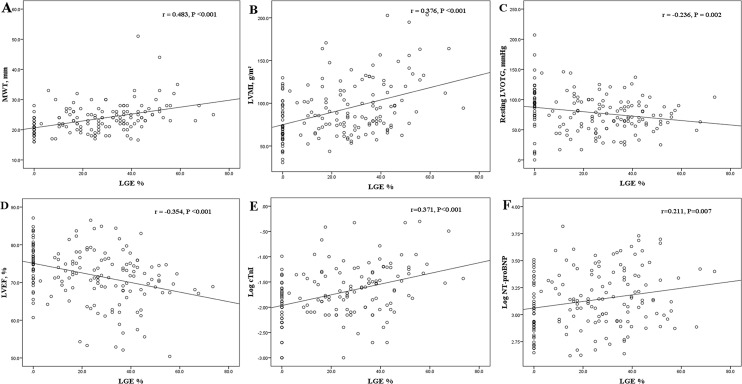
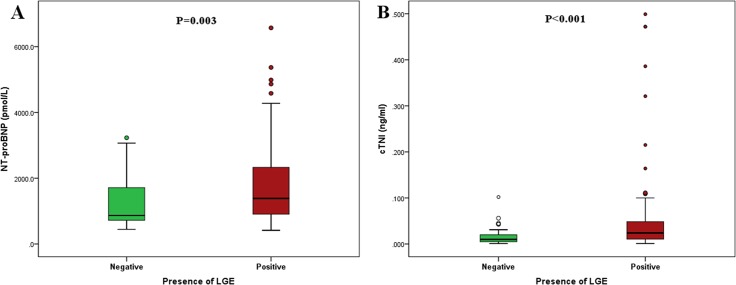
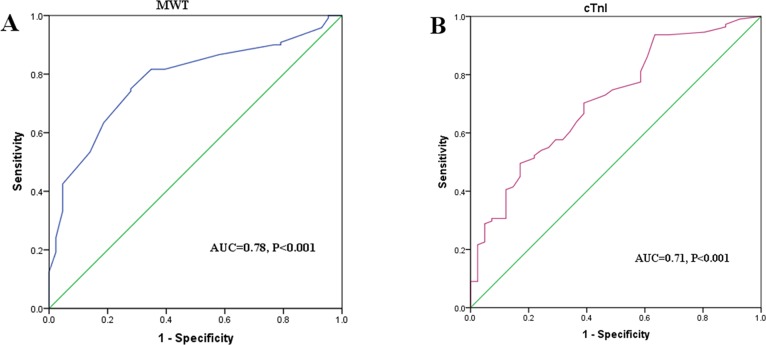
Results: LGE was detected in 120 of 163 patients (73.6%). Patients with LGE had significantly higher levels of NT-proBNP and cTnI than those without LGE (1386.2 [904.6-2340.8] vs. 866.6 [707.2-1875.2] pmol/L, P = 0.003; 0.024 [0.010-0.049] vs. 0.010 [0.005-0.021] ng/ml, P <0.001, respectively). The extent of LGE was positively correlated with log cTnI (r = 0.371, P <0.001) and log NT-proBNP (r = 0.211, P = 0.007). On multivariable analysis, both log cTnI and maximum wall thickness (MWT) were independent predictors of the presence of LGE (OR = 3.193, P = 0.033; OR = 1.410, P < 0.001, respectively), whereas log NT-proBNP was not. According to the ROC curve analysis, combined measurements of MWT ≥21 mm and/or cTnI ≥0.025 ng/ml indicated good diagnostic performance for the presence of LGE, with specificity of 95% or sensitivity of 88%.
Conclusions: Serum cTnI is an independent predictor useful for identifying myocardial fibrosis, while plasma NT-proBNP is only associated with myocardial fibrosis on univariate analysis. Combined measurements of serum cTnI with MWT further improve its value in detecting myocardial fibrosis in patients with HOCM.
Conflict of interest statement
Figures
Similar articles
-
Predictive Values of Apelin for Myocardial Fibrosis in Hypertrophic Cardiomyopathy.Int Heart J. 2019 May 30;60(3):648-655. doi: 10.1536/ihj.18-598. Epub 2019 Apr 25. Int Heart J. 2019. PMID: 31019180
-
Predictive values of multiple non-invasive markers for myocardial fibrosis in hypertrophic cardiomyopathy patients with preserved ejection fraction.Sci Rep. 2021 Feb 22;11(1):4297. doi: 10.1038/s41598-021-83678-z. Sci Rep. 2021. PMID: 33619345 Free PMC article.
-
[Analysis on related factors of myocardial fibrosis in patients with hypertrophic cardiomyopathy].Zhonghua Xin Xue Guan Bing Za Zhi. 2021 Jan 11;49(1):31-36. doi: 10.3760/cma.j.cn112148-20200609-00475. Online ahead of print. Zhonghua Xin Xue Guan Bing Za Zhi. 2021. PMID: 33429483 Chinese.
-
Cardiac Biomarker Release After Exercise in Healthy Children and Adolescents: A Systematic Review and Meta-Analysis.Pediatr Exerc Sci. 2019 Feb 1;31(1):28-36. doi: 10.1123/pes.2018-0058. Epub 2018 Sep 30. Pediatr Exerc Sci. 2019. PMID: 30269651
-
Delayed Diagnosis and Recovery of Fulminant Immune Checkpoint Inhibitor-Associated Myocarditis on VA-ECMO Support.JACC CardioOncol. 2022 Dec 20;4(5):722-726. doi: 10.1016/j.jaccao.2022.08.013. eCollection 2022 Dec. JACC CardioOncol. 2022. PMID: 36636445 Free PMC article. Review.
Cited by
-
Serum N-terminal pro-B-type natriuretic peptide levels are associated with left atrial dilation, resting left ventricular outflow tract gradient, and pulmonary hypertension in patients with hypertrophic cardiomyopathy.Postepy Kardiol Interwencyjnej. 2020 Mar;16(1):97-101. doi: 10.5114/aic.2019.91516. Epub 2020 Feb 9. Postepy Kardiol Interwencyjnej. 2020. PMID: 32368242 Free PMC article.
-
Obstructive Form of Hypertrophic Cardiomyopathy-Left Ventricular Outflow Tract Gradient: Novel Methods of Provocation, Monitoring of Biomarkers, and Recent Advances in the Treatment.Biomed Res Int. 2016;2016:1575130. doi: 10.1155/2016/1575130. Epub 2016 May 10. Biomed Res Int. 2016. PMID: 27247935 Free PMC article. Review.
-
The association of left ventricular histologically verified myocardial fibrosis with pulmonary hypertension in severe aortic stenosis.Perfusion. 2023 Jan;38(1):165-171. doi: 10.1177/02676591211042733. Epub 2021 Sep 15. Perfusion. 2023. PMID: 34524051 Free PMC article.
-
Myocardial bridging in obstructive hypertrophic cardiomyopathy: a risk factor for myocardial fibrosis.BMC Med. 2024 Feb 27;22(1):86. doi: 10.1186/s12916-024-03301-6. BMC Med. 2024. PMID: 38413945 Free PMC article.
-
Diagnostic utility of cardiac troponin I in cats with hypertrophic cardiomyopathy.J Vet Intern Med. 2018 May;32(3):922-929. doi: 10.1111/jvim.15131. Epub 2018 Apr 16. J Vet Intern Med. 2018. PMID: 29660794 Free PMC article.
References
-
- Ho CY, Lopez B, Coelho-Filho OR, Lakdawala NK, Cirino AL, Jarolim P, et al. Myocardial fibrosis as an early manifestation of hypertrophic cardiomyopathy. The New England journal of medicine. 2010;363(6):552–63. Epub 2010/09/08. 10.1056/NEJMoa1002659 ; PubMed Central PMCID: PMCPmc3049917. - DOI - PMC - PubMed
-
- Steggerda RC, Damman K, Balt JC, Liebregts M, ten Berg JM, van den Berg MP. Periprocedural complications and long-term outcome after alcohol septal ablation versus surgical myectomy in hypertrophic obstructive cardiomyopathy: a single-center experience. JACC Cardiovascular interventions. 2014;7(11):1227–34. 10.1016/j.jcin.2014.05.023 . - DOI - PubMed
-
- Chan RH, Maron BJ, Olivotto I, Pencina MJ, Assenza GE, Haas T, et al. Prognostic value of quantitative contrast-enhanced cardiovascular magnetic resonance for the evaluation of sudden death risk in patients with hypertrophic cardiomyopathy. Circulation. 2014;130(6):484–95. 10.1161/CIRCULATIONAHA.113.007094 . - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
