

Quantitative IFN-γ and IL-2 Response Associated with Latent Tuberculosis Test Discordance in HIV-infected Pregnant Women
- PMID: 26765255
- PMCID: PMC4910889
- DOI: 10.1164/rccm.201508-1595OC
Quantitative IFN-γ and IL-2 Response Associated with Latent Tuberculosis Test Discordance in HIV-infected Pregnant Women
Abstract
Rationale: Pregnant women with latent tuberculosis infection (LTBI) are at high risk for development of TB, especially if infected with HIV.
Objectives: To assess the performance of LTBI tests in pregnant and postpartum women infected with HIV, investigate the immunology behind discordance in pregnancy, and explore the implications for the development of postpartum TB.
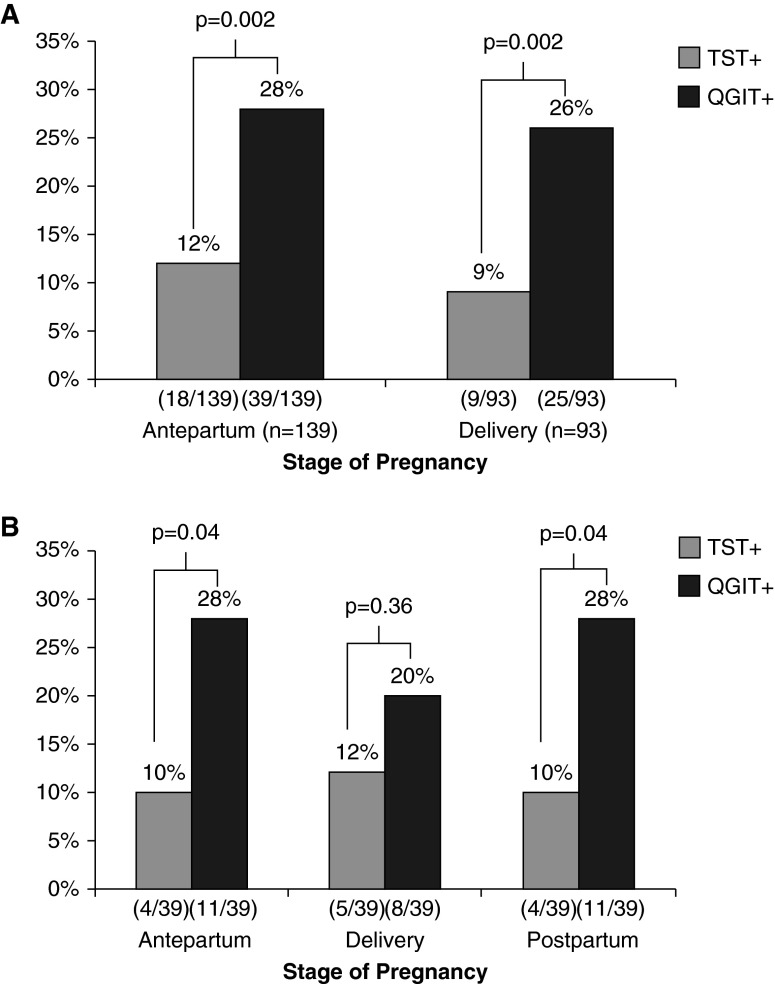
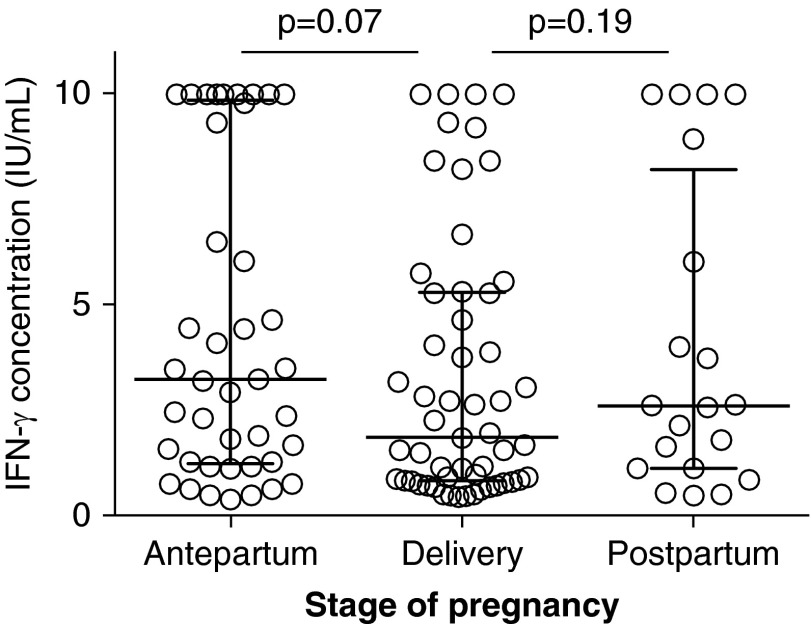
Methods: We screened pregnant women in their second/third trimester and at delivery for LTBI using the tuberculin skin test (TST) and IFN-γ release assay (IGRA) (QuantiFERON Gold). A subset of antepartum women had longitudinal testing, with repeat testing at delivery and postpartum and additional cytokines measured from the IGRA supernatant. The kappa statistic and Wilcoxon rank sum test were used to determine agreement and comparison of cytokine concentrations, respectively.
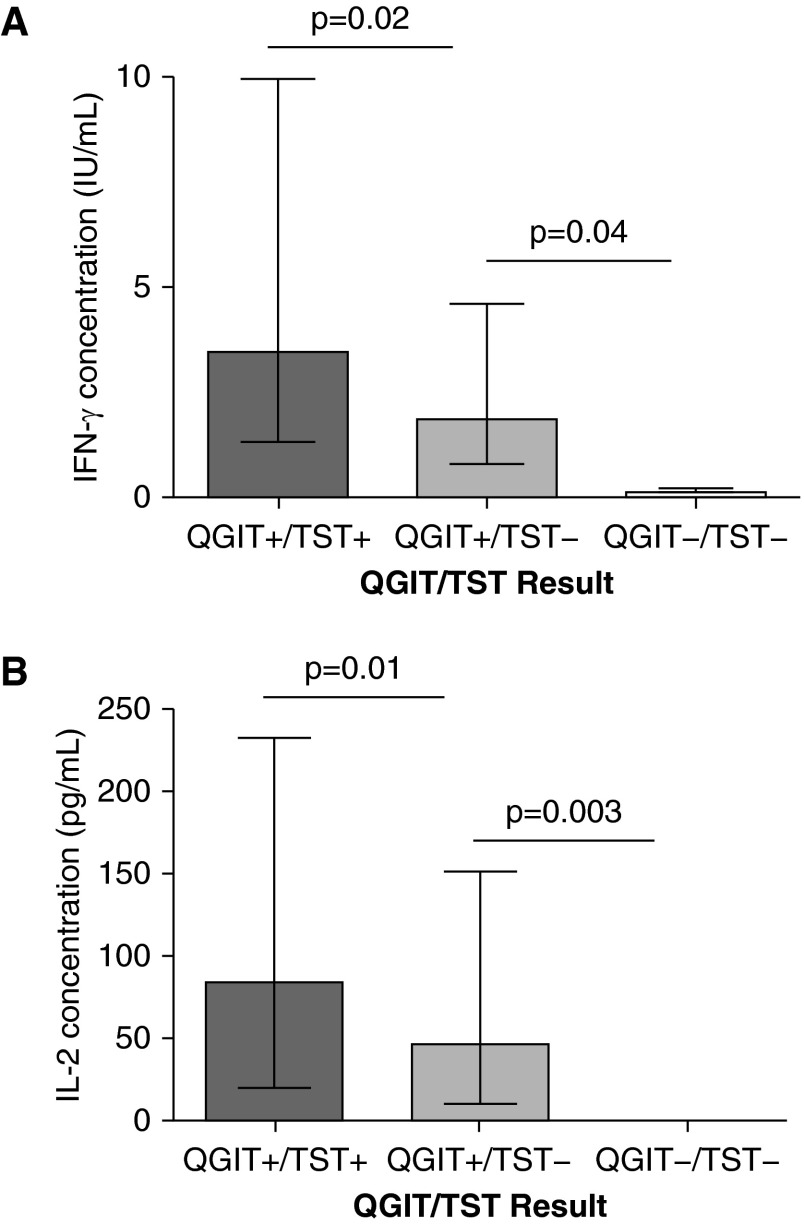
Measurements and main results: Of 252 enrolled, 71 (28%) women had a positive IGRA but only 27 (10%) had a positive TST (P < 0.005). There was 75% agreement (kappa, 0.25). When stratified by pregnancy versus delivery, 20% had IGRA(+)/TST(-) discordance at each time point. A positive IGRA was associated with known TB contact (odds ratio, 3.6; confidence interval, 1.2-11.1; P = 0.02). Compared with IGRA(+)/TST(+), women with IGRA(+)/TST(-) discordance had significantly less IFN-γ (1.85 vs. 3.48 IU/ml; P = 0.02) and IL-2 (46.17 vs. 84.03 pg/ml; P = 0.01). Five developed postpartum TB, of which three had IGRA(+)/TST(-) discordance during pregnancy.
Conclusions: Choice of LTBI test in pregnant women infected with HIV affects results. Pregnant women with IGRA(+)/TST(-) discordance had less IFN-γ and IL-2 than those with concordant-positive results and may represent an especially high-risk subset for the development of active TB postpartum.
Keywords: HIV; IFN-γ release assay; pregnancy; tuberculin skin test; tuberculosis.
Figures
Comment in
-
Diagnosis of Latent Tuberculosis Infection in HIV-infected Pregnant Women. "Baby Steps" toward Better Tuberculosis Control in Pregnancy.Am J Respir Crit Care Med. 2016 Jun 15;193(12):1332-3. doi: 10.1164/rccm.201601-0156ED. Am J Respir Crit Care Med. 2016. PMID: 27304241 No abstract available.
References
-
- World Health Organization. Global tuberculosis report 2014. Geneva: World Health Organization; 2014.
-
- Gupta A, Nayak U, Ram M, Bhosale R, Patil S, Basavraj A, Kakrani A, Philip S, Desai D, Sastry J, et al. Group BJMC-JHUS. Postpartum tuberculosis incidence and mortality among HIV-infected women and their infants in Pune, India, 2002-2005. Nephrol Dial Transplant. 2007;45:241–249. - PubMed
-
- Zenner D, Kruijshaar ME, Andrews N, Abubakar I. Risk of tuberculosis in pregnancy: a national, primary care-based cohort and self-controlled case series study. Am J Respir Crit Care Med. 2012;185:779–784. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
