

Predicting Hemorrhagic Transformation of Acute Ischemic Stroke: Prospective Validation of the HeRS Score
- PMID: 26765425
- PMCID: PMC4718251
- DOI: 10.1097/MD.0000000000002430
Predicting Hemorrhagic Transformation of Acute Ischemic Stroke: Prospective Validation of the HeRS Score
Abstract
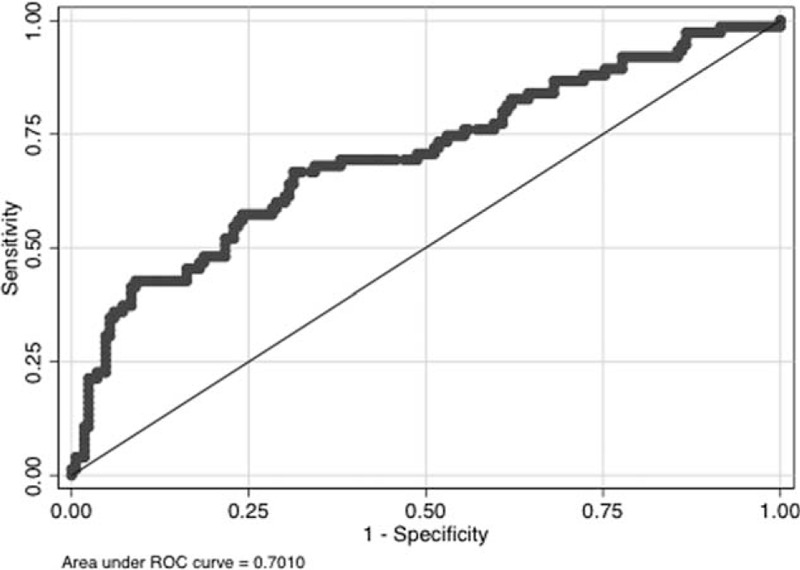
Hemorrhagic transformation (HT) increases the morbidity and mortality of ischemic stroke. Anticoagulation is often indicated in patients with atrial fibrillation, low ejection fraction, or mechanical valves who are hospitalized with acute stroke, but increases the risk of HT. Risk quantification would be useful. Prior studies have investigated risk of systemic hemorrhage in anticoagulated patients, but none looked specifically at HT. In our previously published work, age, infarct volume, and estimated glomerular filtration rate (eGFR) significantly predicted HT. We created the hemorrhage risk stratification (HeRS) score based on regression coefficients in multivariable modeling and now determine its validity in a prospectively followed inpatient cohort.A total of 241 consecutive patients presenting to 2 academic stroke centers with acute ischemic stroke and an indication for anticoagulation over a 2.75-year period were included. Neuroimaging was evaluated for infarct volume and HT. Hemorrhages were classified as symptomatic versus asymptomatic, and by severity. HeRS scores were calculated for each patient and compared to actual hemorrhage status using receiver operating curve analysis.Area under the curve (AUC) comparing predicted odds of hemorrhage (HeRS score) to actual hemorrhage status was 0.701. Serum glucose (P < 0.001), white blood cell count (P < 0.001), and warfarin use prior to admission (P = 0.002) were also associated with HT in the validation cohort. With these variables, AUC improved to 0.854. Anticoagulation did not significantly increase HT; but with higher intensity anticoagulation, hemorrhages were more likely to be symptomatic and more severe.The HeRS score is a valid predictor of HT in patients with ischemic stroke and indication for anticoagulation.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- Jickling GC, Manolescu BN. Breaking down barriers to identifying hemorrhagic transformation in ischemic stroke. Neurology 2012; 79:1632–1633. - PubMed
-
- Khatri P, Wechsler LR, Broderick JP. Intracranial hemorrhage associated with revascularization therapies. Stroke 2007; 38:431–440. - PubMed
-
- Toni D, Fiorelli M, Bastianello S, et al. Hemorrhagic transformation of brain infarct: predictability in the first 5 hours from stroke onset and influence on clinical outcome. Neurology 1996; 46:341–345. - PubMed
-
- Hornig CR, Dorndorf W, Agnoli AL. Hemorrhagic cerebral infarction—a prospective study. Stroke 1986; 17:179–185. - PubMed
-
- Coull BM, Williams LS, Goldstein LB, et al. Anticoagulants and antiplatelet agents in acute ischemic stroke: report of the joint stroke guideline development committee of the American Academy of Neurology and the American Stroke Association (a division of the American Heart Association). Stroke 2002; 33:1934–1942. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
