

Preoperative CT Predicting Recurrence of Surgically Resected Adenocarcinoma of the Lung
- PMID: 26765471
- PMCID: PMC4718297
- DOI: 10.1097/MD.0000000000002513
Preoperative CT Predicting Recurrence of Surgically Resected Adenocarcinoma of the Lung
Abstract
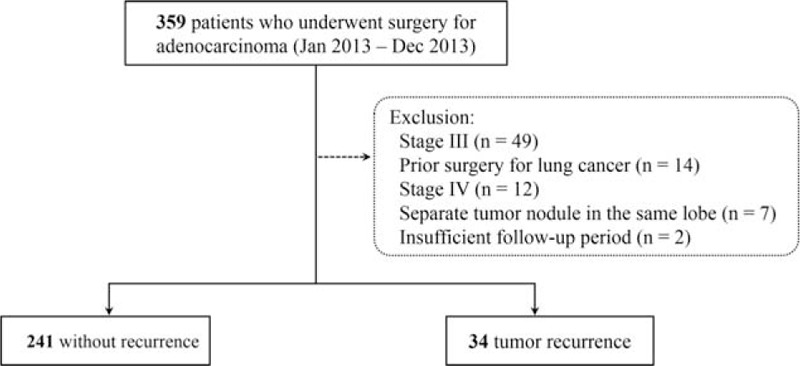
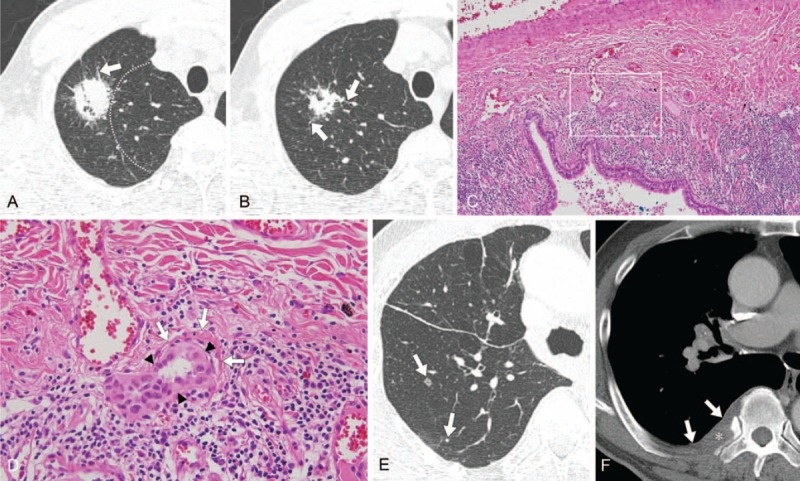
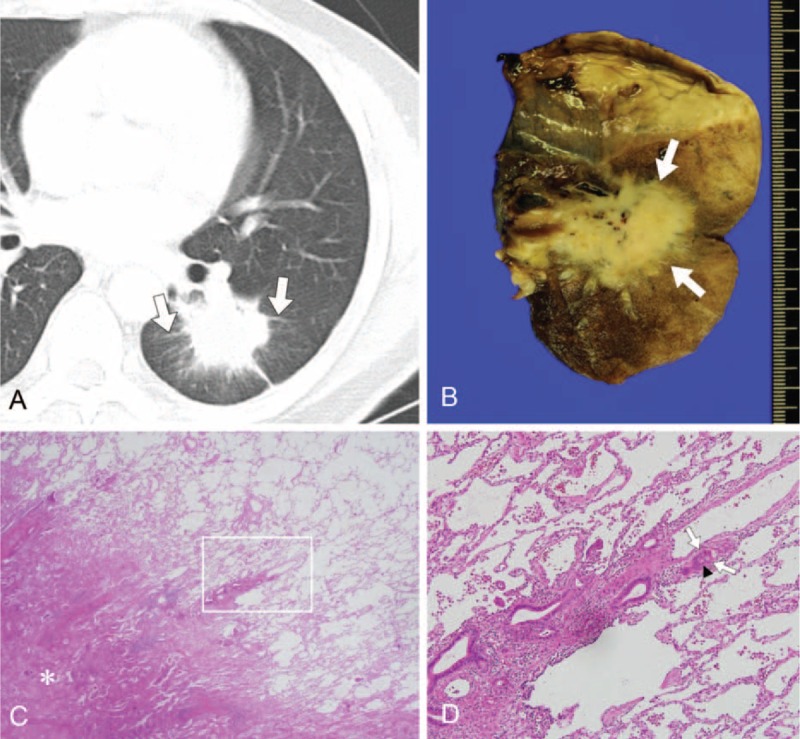
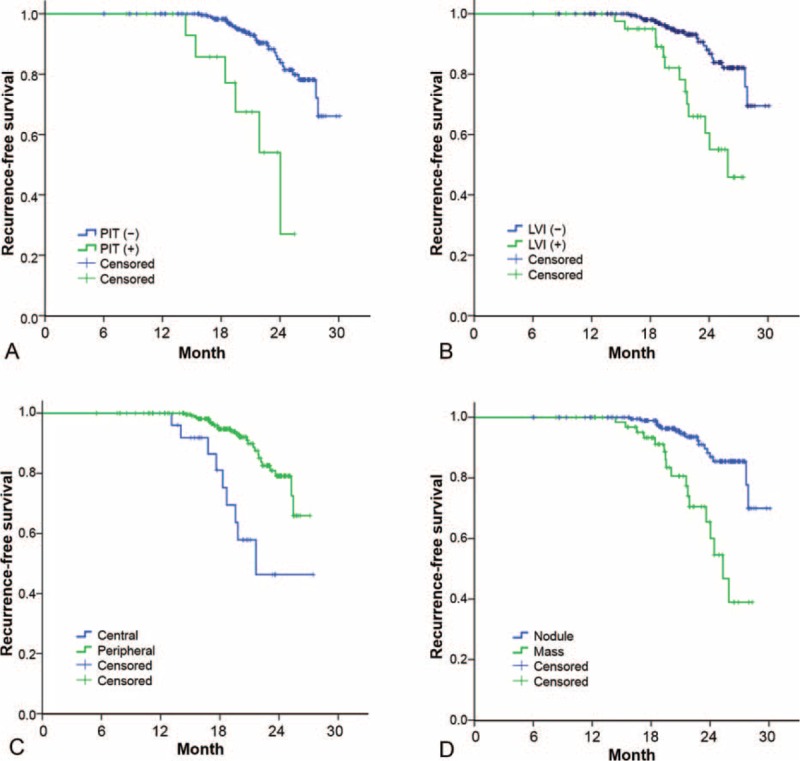
Pathologic lymphovascular invasion (LVI) has been shown to be related to tumor recurrence in lung adenocarcinoma (ADC). We investigated preoperative computed tomography (CT) findings that may be related to pathologic LVI and recurrence of surgically managed stage I-II ADC of the lung.Consecutive patients (n = 275) with ADC from January 2013 to December 2013 were retrospectively enrolled. Two independent chest radiologists analyzed the CT findings. Clinical, CT (stage, margin, pleural tag, axial location, and peritumoral interstitial thickening), and pathologic findings (stage, % lepidic growth, and LVI) were reviewed. Cox proportional hazard regression analysis was used to estimate the hazard ratios (HRs) for patients with (n = 34) and without (n = 241) recurrence.The κ index for agreement on the CT findings between radiologists was 0.705 to 0.845. In univariate analysis, % lepidic growth (P = 0.006), LVI (P < 0.001), size (P < 0.001), and staging (P = 0.011) differentiated significantly between patients with and without recurrence. Long diameter (P < 0.001), mass type (P < 0.001), marginal lobulation (P = 0.020), central location (P < 0.001), and peritumoral interstitial thickening (P < 0.001) were significantly related to recurrence on CT. Peritumoral interstitial thickening was positively correlated with tumor size (P < 0.001), LVI (P < 0.001), N staging (P = 0.005), stage (P < 0.001), mass type (P < 0.001), and recurrence (P = 0.003). In multivariate analysis, size (HR, 1.052; 95% CI, 1.022-1.082; P < 0.001), central location (HR, 3.152; 1.387-7.166; P = 0.006), and LVI (HR, 2.153, 95% CI, 1.038-4.465; P = 0.039) were independent predictors of recurrence.Large, centrally located tumors with LVI tend to recur after surgery. Presence of peritumoral interstitial thickening on CT appears to predict pathologic LVI and recurrence.
Conflict of interest statement
This work supported by research grant from Korean Association for the Study of Lung Cancer in 2015. The authors have no potential conflicts of interest with any companies/organizations whose products or services may be discussed in this article.
The authors have no conflicts of interest to disclose.
Figures
References
-
- Swensen SJ, Jett JR, Hartman TE, et al. CT screening for lung cancer: five-year prospective experience. Radiology 2005; 235:259–265. - PubMed
-
- Goldstraw P, Crowley J, Chansky K, et al. The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of malignant tumours. J Thorac Oncol 2007; 2:706–714. - PubMed
-
- Chansky K, Sculier JP, Crowley JJ, et al. The International Association for the Study of Lung Cancer Staging Project: prognostic factors and pathologic TNM stage in surgically managed non-small cell lung cancer. J Thorac Oncol 2009; 4:792–801. - PubMed
-
- Yang HC, Kim HR, Jheon S, et al. Recurrence risk-scoring model for stage I adenocarcinoma of the lung. Ann Surg Oncol 2015; 22:4089–4097. - PubMed
-
- Kodama K, Higashiyama M, Yokouchi H, et al. Prognostic value of ground-glass opacity found in small lung adenocarcinoma on high-resolution CT scanning. Lung Cancer 2001; 33:17–25. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
