

Comparative Effectiveness of Emergency Resuscitative Thoracotomy versus Closed Chest Compressions among Patients with Critical Blunt Trauma: A Nationwide Cohort Study in Japan
- PMID: 26766574
- PMCID: PMC4713157
- DOI: 10.1371/journal.pone.0145963
Comparative Effectiveness of Emergency Resuscitative Thoracotomy versus Closed Chest Compressions among Patients with Critical Blunt Trauma: A Nationwide Cohort Study in Japan
Abstract
Background: Although emergency resuscitative thoracotomy is performed as a salvage maneuver for critical blunt trauma patients, evidence supporting superior effectiveness of emergency resuscitative thoracotomy compared to conventional closed-chest compressions remains insufficient. The objective of this study was to investigate whether emergency resuscitative thoracotomy at the emergency department or in the operating room was associated with favourable outcomes after blunt trauma and to compare its effectiveness with that of closed-chest compressions.
Methods: This was a retrospective nationwide cohort study. Data were obtained from the Japan Trauma Data Bank for the period between 2004 and 2012. The primary and secondary outcomes were patient survival rates 24 h and 28 d after emergency department arrival. Statistical analyses were performed using multivariable generalized mixed-effects regression analysis. We adjusted for the effects of different hospitals by introducing random intercepts in regression analysis to account for the differential quality of emergency resuscitative thoracotomy at hospitals where patients in cardiac arrest were treated. Sensitivity analyses were performed using propensity score matching.
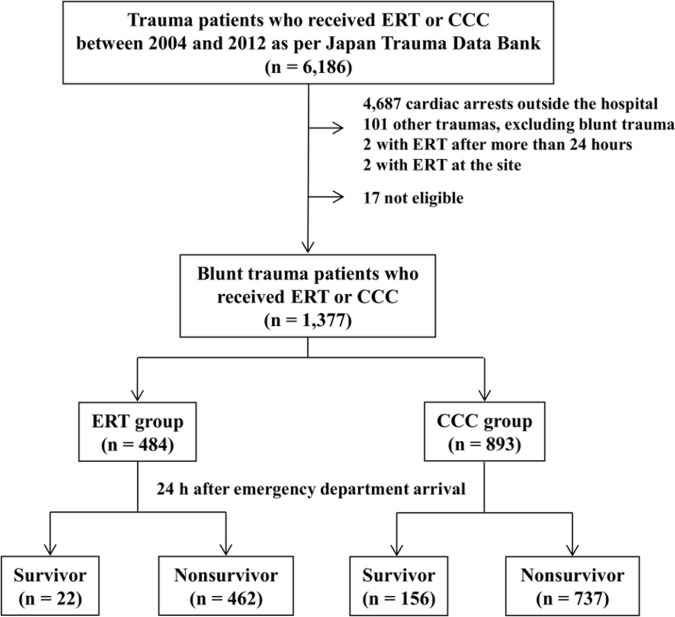
Results: In total, 1,377 consecutive, critical blunt trauma patients who received cardiopulmonary resuscitation in the emergency department or operating room were included in the study. Of these patients, 484 (35.1%) underwent emergency resuscitative thoracotomy and 893 (64.9%) received closed-chest compressions. Compared to closed-chest compressions, emergency resuscitative thoracotomy was associated with lower survival rate 24 h after emergency department arrival (4.5% vs. 17.5%, respectively, P < 0.001) and 28 d after arrival (1.2% vs. 6.0%, respectively, P < 0.001). Multivariable generalized mixed-effects regression analysis with and without a propensity score-matched dataset revealed that the odds ratio for an unfavorable survival rate after 24 h was lower for emergency resuscitative thoracotomy than for closed-chest compressions (P < 0.001).
Conclusions: Emergency resuscitative thoracotomy was independently associated with decreased odds of a favorable survival rate compared to closed-chest compressions.
Conflict of interest statement
Figures
References
-
- Fingerhut LA, Warner M. Injury chartbook. Health, United States, 1996–1997. Hyattsville, Maryland: National Center for Health Statistics; 1997.
-
- Shackford SR, Hollingworth-Fridlund P, Cooper GF, Eastman AB. The effect of regionalization upon the quality of trauma care as assessed by concurrent audit before and after institution of a trauma system: a preliminary report. J Trauma. 1986;26: 812–820. - PubMed
-
- West JG, Trunkey DD, Lim RC. Systems of trauma care. A study of two counties. Arch Surg. 1979;114: 455–460. - PubMed
-
- Arreola-Risa C, Mock CN, Lojero-Wheatly L, de la Cruz O, Garcia C, Canavati-Ayub F, et al. Low-cost improvements in prehospital trauma care in a Latin American city. J Trauma. 2000;48: 119–124. - PubMed
-
- Injuries and violence: the facts WHO Press; 2010. Available: http://www.who.int/violence_injury_prevention/key_facts/en/.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
