

CT angiography and CT perfusion improve prediction of infarct volume in patients with anterior circulation stroke
- PMID: 26767380
- PMCID: PMC4819789
- DOI: 10.1007/s00234-015-1636-z
CT angiography and CT perfusion improve prediction of infarct volume in patients with anterior circulation stroke
Abstract
Introduction: We investigated whether baseline CT angiography (CTA) and CT perfusion (CTP) in acute ischemic stroke could improve prediction of infarct presence and infarct volume on follow-up imaging.
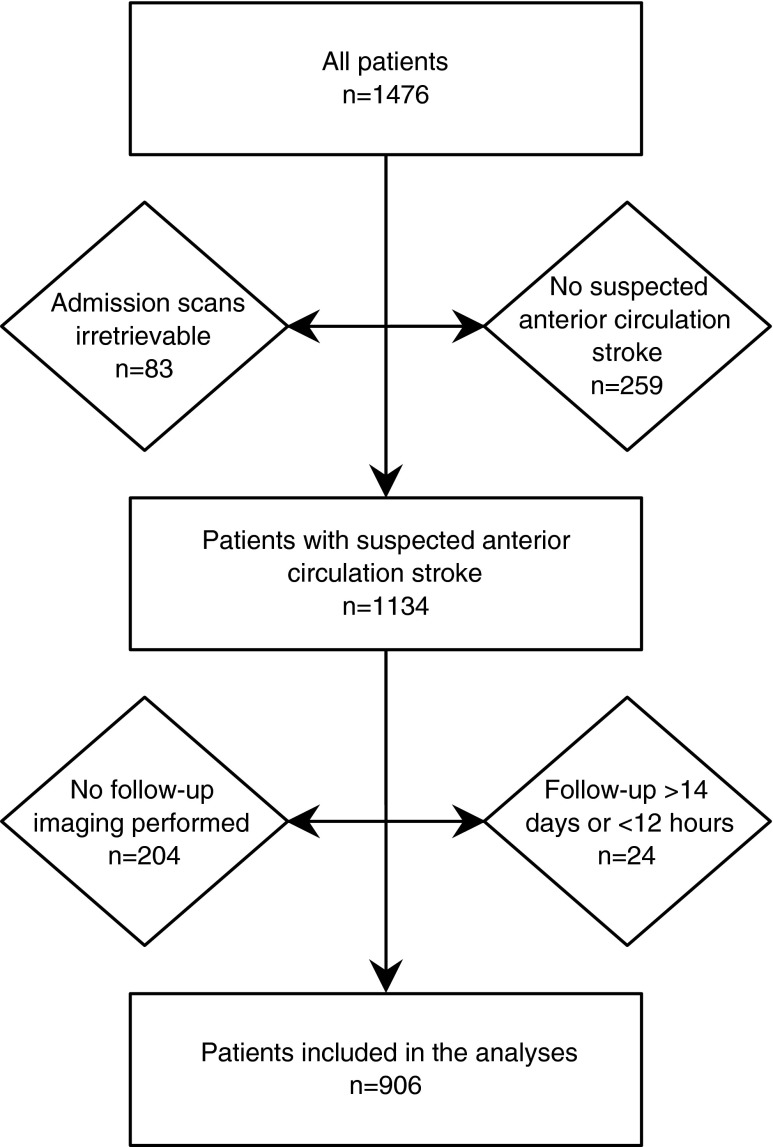
Methods: We analyzed 906 patients with suspected anterior circulation stroke from the prospective multicenter Dutch acute stroke study (DUST). All patients underwent baseline non-contrast CT, CTA, and CTP and follow-up non-contrast CT/MRI after 3 days. Multivariable regression models were developed including patient characteristics and non-contrast CT, and subsequently, CTA and CTP measures were added. The increase in area under the curve (AUC) and R (2) was assessed to determine the additional value of CTA and CTP.
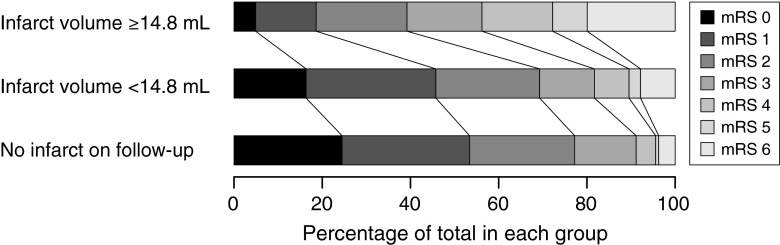
Results: At follow-up, 612 patients (67.5%) had a detectable infarct on CT/MRI; median infarct volume was 14.8 mL (interquartile range (IQR) 2.8-69.6). Regarding infarct presence, the AUC of 0.82 (95% confidence interval (CI) 0.79-0.85) for patient characteristics and non-contrast CT was improved with addition of CTA measures (AUC 0.85 (95% CI 0.82-0.87); p < 0.001) and was even higher after addition of CTP measures (AUC 0.89 (95% CI 0.87-0.91); p < 0.001) and combined CTA/CTP measures (AUC 0.89 (95% CI 0.87-0.91); p < 0.001). For infarct volume, adding combined CTA/CTP measures (R (2) = 0.58) was superior to patient characteristics and non-contrast CT alone (R (2) = 0.44) and to addition of CTA alone (R (2) = 0.55) or CTP alone (R (2) = 0.54; all p < 0.001).
Conclusion: In the acute stage, CTA and CTP have additional value over patient characteristics and non-contrast CT for predicting infarct presence and infarct volume on follow-up imaging. These findings could be applied for patient selection in future trials on ischemic stroke treatment.
Keywords: CT angiography; CT perfusion; Infarct volume; Ischemic stroke; Prediction.
Figures

References
-
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Magid D, Marcus GM, Marelli A, Matchar DB, McGuire DK, Mohler ER, Moy CS, Mussolino ME, Nichol G, Paynter NP, Schreiner PJ, Sorlie PD, Stein J, Turan TN, Virani SS, Wong ND, Woo D, Turner MB. Heart disease and stroke statistics—2013 update: a report from the American Heart Association. Circulation. 2013;127:e6–e245. doi: 10.1161/CIR.0b013e31828124ad. - DOI - PMC - PubMed
-
- Berkhemer OA, Fransen PS, Beumer D, van den Berg LA, Lingsma HF, Yoo AJ, Schonewille WJ, Vos JA, Nederkoorn PJ, Wermer MJ, van Walderveen MA, Staals J, Hofmeijer J, van Oostayen JA, Lycklama A, Nijeholt GJ, Brouwer PA, Emmer BJ, de Bruijn SF, van Dijk LC, Kappelle LJ, Lo RH, van Dijk EJ, de Vries J, de Kort PL, van Rooij WJ, van den Berg JS, van Hasselt BA, Aerden LA, Dallinga RJ, Visser MC, Bot JC, Vroomen PC, Eshghi O, Schreuder TH, Heijboer RJ, Keizer K, Tielbeek AV, den Hertog HM, Gerrits DG, van den Berg-Vos RM, Karas GB, Steyerberg EW, Flach HZ, Marquering HA, Sprengers ME, Jenniskens SF, Beenen LF, van den Berg R, Koudstaal PJ, van Zwam WH, Roos YB, van der Lugt A, van Oostenbrugge RJ, Majoie CB, Dippel DW. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015;372:11–20. doi: 10.1056/NEJMoa1411587. - DOI - PubMed
-
- Jovin TG, Chamorro A, Cobo E, de Miquel MA, Molina CA, Rovira A, San Roman L, Serena J, Abilleira S, Ribo M, Millan M, Urra X, Cardona P, Lopez-Cancio E, Tomasello A, Castano C, Blasco J, Aja L, Dorado L, Quesada H, Rubiera M, Hernandez-Perez M, Goyal M, Demchuk AM, von Kummer R, Gallofre M, Davalos A. Thrombectomy within 8 hours after symptom onset in ischemic stroke. N Engl J Med. 2015;372:2296–2306. doi: 10.1056/NEJMoa1503780. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
