

Phyllodes tumours of the breast: a consensus review
- PMID: 26768026
- PMCID: PMC5027876
- DOI: 10.1111/his.12876
Phyllodes tumours of the breast: a consensus review
Abstract
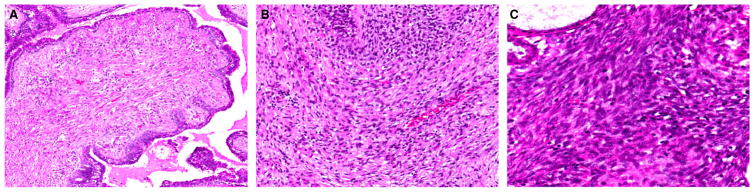
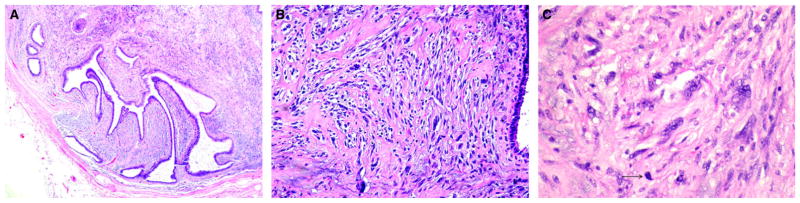
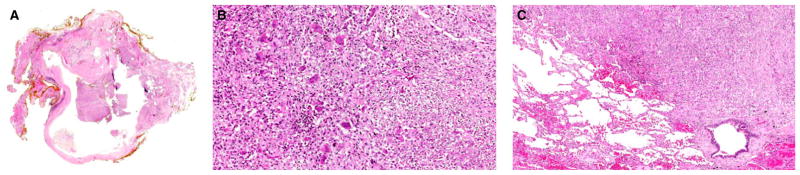
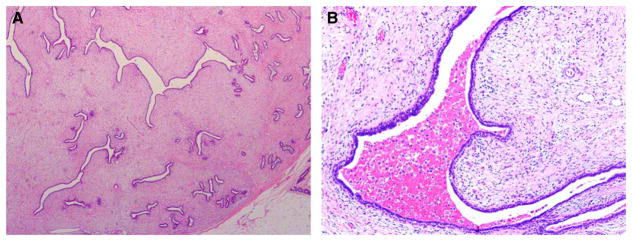
Phyllodes tumours constitute an uncommon but complex group of mammary fibroepithelial lesions. Accurate and reproducible grading of these tumours has long been challenging, owing to the need to assess multiple stratified histological parameters, which may be weighted differently by individual pathologists. Distinction of benign phyllodes tumours from cellular fibroadenomas is fraught with difficulty, due to overlapping microscopic features. Similarly, separation of the malignant phyllodes tumour from spindle cell metaplastic carcinoma and primary breast sarcoma can be problematic. Phyllodes tumours are treated by surgical excision. However, there is no consensus on the definition of an appropriate surgical margin to ensure completeness of excision and reduction of recurrence risk. Interpretive subjectivity, overlapping histological diagnostic criteria, suboptimal correlation between histological classification and clinical behaviour and the lack of robust molecular predictors of outcome make further investigation of the pathogenesis of these fascinating tumours a matter of active research. This review consolidates the current understanding of their pathobiology and clinical behaviour, and includes proposals for a rational approach to the classification and management of phyllodes tumours.
Keywords: classification; fibroadenoma; malignant; metastasis; phyllodes.
© 2015 John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest with respect to the authorship, research and/or publication of this article
Figures

References
-
- Lakhani SR, Ellis IO, Schnitt SJ, Tan PH, van de Vijver MJ, editors. World Health Organization Classification of Tumours of the Breast. Lyon: IARC Press; 2012.
-
- Azzopardi J. Problems in Breast Pathology. London: WB Saunders; 1979. pp. 346–365. - PubMed
-
- Jara-Lazaro AR, Akhilesh M, Thike AA, Lui PC-W, Tse GM-K, Tan PH. Predictors of phyllodes tumours on core biopsy specimens of fibroepithelial neoplasms. Histopathology. 2010;57:220–232. - PubMed
-
- Tan PH, Thike AA, Tan WJ, et al. Predicting clinical behaviour of breast phyllodes tumours: a nomogram based on histological criteria and surgical margins. J Clin Pathol. 2012;65:69–76. - PubMed
-
- Tsang JYS, Ni Y-B, Ng EK, et al. MicroRNAs are differentially deregulated in mammary malignant phyllodes tumour. Histopathology. 2015;67:294–305. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
