

Design and analysis considerations in the Ebola_Tx trial evaluating convalescent plasma in the treatment of Ebola virus disease in Guinea during the 2014-2015 outbreak
- PMID: 26768570
- PMCID: PMC4738238
- DOI: 10.1177/1740774515621056
Design and analysis considerations in the Ebola_Tx trial evaluating convalescent plasma in the treatment of Ebola virus disease in Guinea during the 2014-2015 outbreak
Abstract
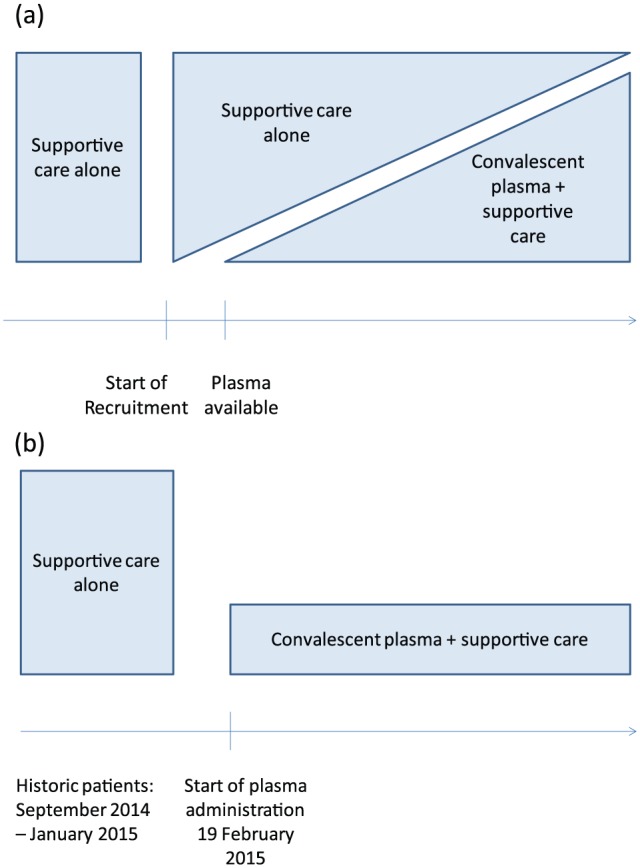
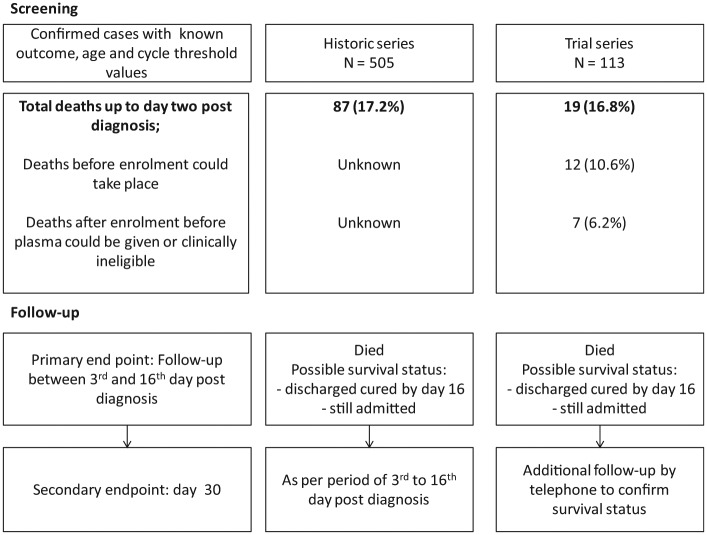
The Ebola virus disease outbreak in 2014-2015 led to a huge caseload with a high case fatality rate. No specific treatments were available beyond supportive care for conditions such as dehydration and shock. Evaluation of treatment with convalescent plasma from Ebola survivors was identified as a priority. We evaluated this intervention in an emergency setting, where randomization was unacceptable. The original trial design was an open-label study comparing patients receiving convalescent plasma and supportive care to patients receiving supportive care alone. The comparison group comprised patients recruited at the start of the trial before convalescent plasma became available, as well as patients presenting during the trial for whom there was insufficient blood group-compatible plasma or no staffing capacity to provide additional transfusions. However, during the trial, convalescent plasma was available to treat all new patients. The design was changed to use a comparator group comprising patients previously treated at the same Ebola treatment center prior to the start of the trial. In the analysis, it was planned to adjust for any differences in prognostic variables between intervention and comparison groups, specifically baseline polymerase chain reaction cycle threshold and age. In addition, adjustment was planned for other potential confounders, identified in the analysis, such as patient presenting symptoms and time to treatment seeking. Because plasma treatment started up to 3 days after diagnosis and we could not define a similar time-point for the comparator group, patients who died before the third day after confirmation of diagnosis were excluded from both intervention and comparison groups in a per-protocol analysis. Some patients received additional experimental treatments soon after plasma treatment, and these were excluded. We also analyzed mortality including all patients from the time of confirmed diagnosis, irrespective of whether those in the trial series actually received plasma, as an intention-to-treat analysis. Per-protocol and intention-to-treat approaches gave similar conclusions. An important caveat in the interpretation of the findings is that it is unlikely that all potential sources of confounding, such as any variation in supportive care over time, were eliminated. Protocols and electronic data capture systems have now been extensively field-tested for emergency evaluation of treatment with convalescent plasma. Ongoing studies seek to quantify the level of neutralizing antibodies in different plasma donations to determine whether this influences the response and survival of treated patients.
Trial registration: ClinicalTrials.gov NCT02342171.
Keywords: Ebola; Guinea; convalescent plasma; trial design.
© The Author(s) 2016.
Conflict of interest statement
Figures
References
-
- Casadevall A, Dadachova E, Pirofski LA. Passive antibody therapy for infectious diseases. Nat Rev Microbiol 2004; 2: 695–703. - PubMed
-
- Mupapa K, Massamba M, Kibadi K, et al. Treatment of Ebola hemorrhagic fever with blood transfusions from convalescent patients. J Infect Dis 1999; 179: S18–S23. - PubMed
-
- Gulland A. First Ebola treatment is approved by WHO. BMJ 2014; 349: g5539. - PubMed
-
- Maurice J. WHO meeting chooses untried interventions to defeat Ebola. Lancet 2014; 384: e45–e46. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
