

Infused total nucleated cell dose is a better predictor of transplant outcomes than CD34+ cell number in reduced-intensity mobilized peripheral blood allogeneic hematopoietic cell transplantation
- PMID: 26768686
- PMCID: PMC5004400
- DOI: 10.3324/haematol.2015.134841
Infused total nucleated cell dose is a better predictor of transplant outcomes than CD34+ cell number in reduced-intensity mobilized peripheral blood allogeneic hematopoietic cell transplantation
Abstract
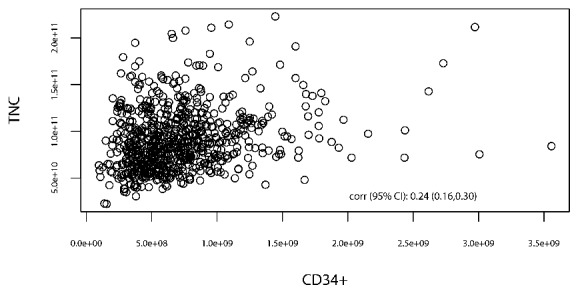
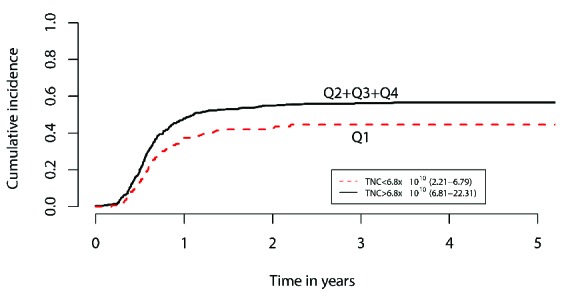
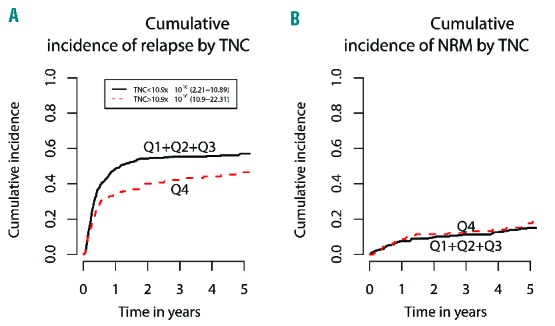
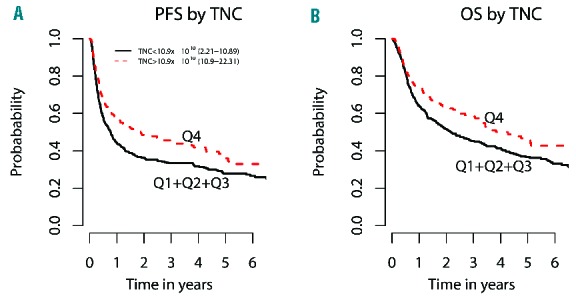
Mobilized peripheral blood is the most common graft source for allogeneic hematopoietic stem cell transplantation following reduced-intensity conditioning. In assessing the effect of donor cell dose and graft composition on major transplant outcomes in the reduced-intensity setting, prior studies focused primarily on CD34(+)cell dose and reported conflicting results, especially in relation to survival end-points. While the impact of total nucleated cell dose has been less frequently evaluated, available studies suggest higher total nucleated cell dose is associated with improved survival outcomes in the reduced-intensity setting. In order to further explore the relationship between CD34(+)cell dose and total nucleated cell dose on reduced-intensity transplant outcomes, we analyzed the effect of donor graft dose and composition on outcomes of 705 patients with hematologic malignancies who underwent reduced-intensity peripheral blood stem cell transplantation at the Dana Farber Cancer Institute from 2000 to 2010. By multivariable analysis we found that higher total nucleated cell dose (top quartile; ≥10.8 × 10(10)cells) was associated with improved overall survival [HR 0.69 (0.54-0.88),P=0.0028] and progression-free survival [HR 0.68 (0.54-0.85),P=0.0006]. Higher total nucleated cell dose was independently associated with decreased relapse [HR 0.66 (0.51-0.85),P=0.0012] and increased incidence of chronic graft-versus-host disease [HR 1.4 (1.12-1.77),P=0.0032]. In contrast, higher doses of CD34(+)cells (top quartile; ≥10.9 × 10(6)/kg) had no significant effect on graft-versus-host disease or survival outcomes. These data suggest total nucleated cell dose is a more relevant prognostic variable for reduced-intensity transplant outcomes than the more commonly studied CD34(+)cell dose.
Copyright© Ferrata Storti Foundation.
Figures
References
-
- Perez-Simon JA, Diez-Campelo M, Martino R, et al. Impact of CD34+ cell dose on the outcome of patients undergoing reduced-intensity-conditioning allogeneic peripheral blood stem cell transplantation. Blood. 2003;102(3):1108–1113. - PubMed
-
- Panse JP, Heimfeld S, Guthrie KA, et al. Allogeneic peripheral blood stem cell graft composition affects early T-cell chimaerism and later clinical outcomes after non-myeloablative conditioning. Br J Haematol. 2005;128(5):659–667. - PubMed
-
- Mehta J, Frankfurt O, Altman J, et al. Optimizing the CD34+ cell dose for reduced-intensity allogeneic hematopoietic stem cell transplantation. Leuk Lymphoma. 2009;50(9):1434–1441. - PubMed
-
- Tsirigotis P, Shapira MY, Or R, et al. The number of infused CD34+ cells does not influence the incidence of GVHD or the outcome of allogeneic PBSC transplantation, using reduced-intensity conditioning and antithymocyte globulin. Bone Marrow Transplant. 2010;45(7):1189–1196. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
