

Repeat transcatheter aortic valve implantation using a latest generation balloon-expandable device for treatment of failing transcatheter heart valves
- PMID: 26768837
- PMCID: PMC4714508
- DOI: 10.1186/s13019-016-0398-y
Repeat transcatheter aortic valve implantation using a latest generation balloon-expandable device for treatment of failing transcatheter heart valves
Abstract
Background: Paravalvular leakage (PVL) is a known complication of transcatheter aortic valve implantation (TAVI) and is associated with poor outcome. Besides balloon-post-dilatation, valve-in-valve (ViV) procedures can be taken into consideration to control this complication. Herein we present initial experience with use of the latest generation balloon-expandable Edwards Sapien 3® (S3) transcatheter heart valve (THV) for treatment of failing THVs.
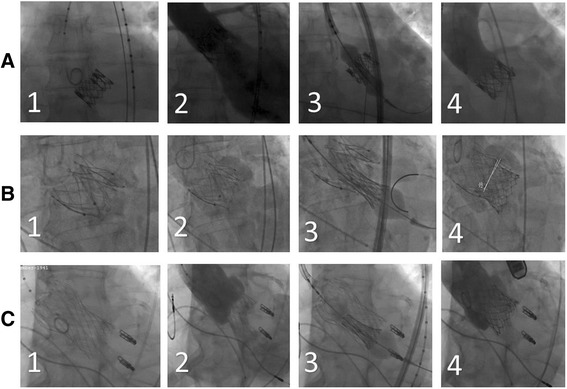
Methods: Between 01/2014 and 12/2014 three patients (two male, age: 71-80 y, log EUROScore I: 11.89 - 32.63) with failing THVs were refered to our institution for further treatment. THV approach with secondary implantation of an S3 was chosen after mutual agreement of the local interdisciplinary heart team at an interval of 533-1119 days from the index procedure. The performed procedures consisted of: S3 in Sapien XT, JenaValve and CoreValve.
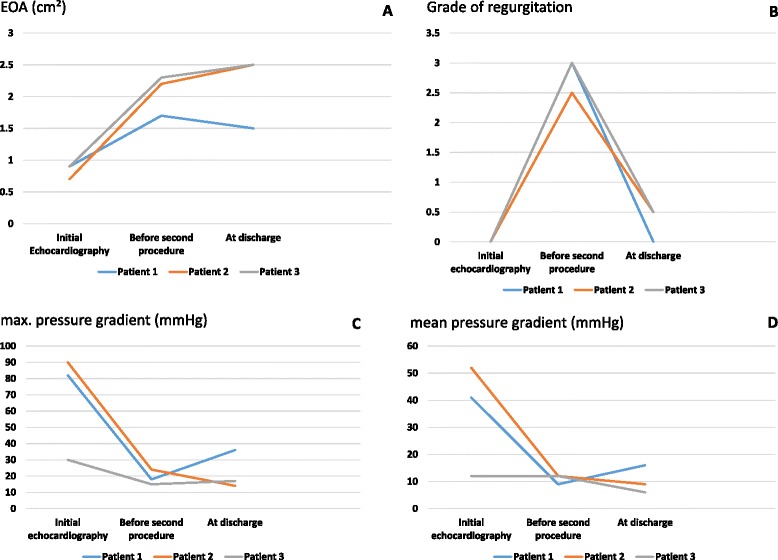
Results: Successful transfemoral implantation with significant reduction of PVL was achieved in all cases. No intraprocedural complications occurred regarding placement of the S3 with a postprocedural effective orifice area (EOA) of 1.5-2.5 cm(2) and pressure gradients of max/mean 14/6-36/16 mmHg. 30-day mortality was 0%. At the latest follow-up of 90-530 days, all patients are alive and well with satisfactory THV function. Regarding VARC-2 criteria one major bleeding and one TIA was reported.
Conclusions: In the instance of moderate or severe aortic regurgitation after TAVI, S3 ViV deployment is an excellent option to reduce residual regurgitation to none or mild. For further assertions concerning functional outcomes long-term results have to be awaited.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
