

Clinical and economic burden associated with cardiovascular events among patients with hyperlipidemia: a retrospective cohort study
- PMID: 26769473
- PMCID: PMC4714430
- DOI: 10.1186/s12872-016-0190-x
Clinical and economic burden associated with cardiovascular events among patients with hyperlipidemia: a retrospective cohort study
Abstract
Background: Annual direct costs for cardiovascular (CV) diseases in the United States are approximately $195.6 billion, with many high-risk patients remaining at risk for major cardiovascular events (CVE). This study evaluated the direct clinical and economic burden associated with new CVE up to 3 years post-event among patients with hyperlipidemia.
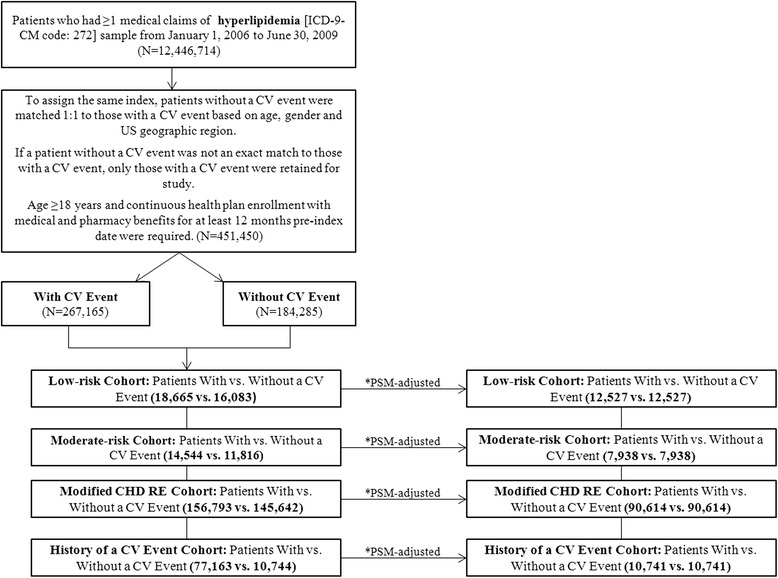
Methods: Hyperlipidemic patients with a primary inpatient claim for new CVE (myocardial infarction, unstable angina, ischemic stroke, transient ischemic attack, coronary artery bypass graft, percutaneous coronary intervention and heart failure) were identified using IMS LifeLink PharMetrics Plus data from January 1, 2006 through June 30, 2012. Patients were stratified by CV risk into history of CVE, modified coronary heart disease risk equivalent, moderate- and low-risk cohorts. Of the eligible patients, propensity score matched 243,640 patients with or without new CVE were included to compare healthcare resource utilization and direct costs ranging from the acute (1-month) phase through 3 years post-CVE date (follow-up period).
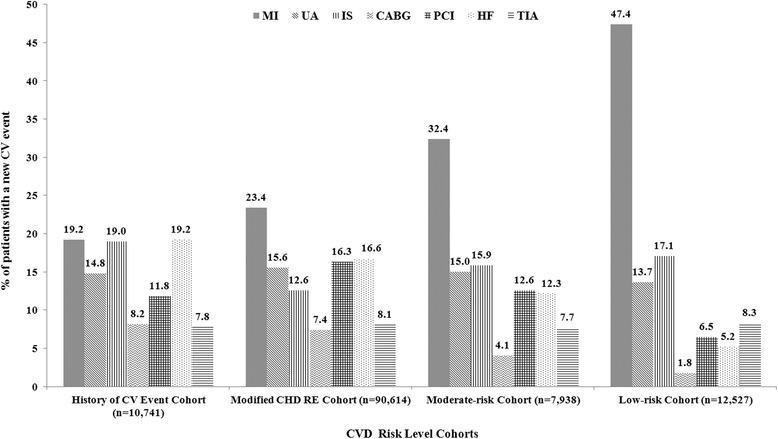
Results: Myocardial infarction was the most common CVE in all the risk cohorts. During the acute phase, among patients with new CVE, the average incremental inpatient length of stay and incremental costs ranged from 4.4-6.2 days and $25,666-$30,321, respectively. Acute-phase incremental costs accounted for 61-75% of first-year costs, but incremental costs also remained high during years 2 and 3 post-CVE.
Conclusions: Among hyperlipidemic patients with new CVE, healthcare utilization and costs incurred were significantly higher than for those without CVE during the acute phase, and remained higher up to 3 years post-event, across all risk cohorts.
Figures
References
-
- Bloom DE, Cafiero ET, Jané-Llopis E, Abrahams-Gessel S, Bloom LR, Fathima S, et al., editors. The Global Economic Burden of Non-communicable Diseases. Geneva: World Economic Forum; 2011.
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee: Heart disease and stroke statistics--2015 update: A report from the American Heart Association. Circulation. 2015;131:e29–e322. doi: 10.1161/CIR.0000000000000152. - DOI - PubMed
-
- Soni A. Top 10 most costly condition among men and women 2008: estimates for the U.S. civilian noninstitutionalized adult population, age 18 and older. Medical Expenditure Panel Survey. Statistical Brief #331. http://meps.ahrq.gov/mepsweb/data_files/publications/st331/stat331.shtml. Accessed 14 July 2014.
-
- Willerson JT, Ridker PM. Inflammation as a cardiovascular risk factor. Circulation. 2004;109(21 Suppl 1):II2–10. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
