

eGFR and Outcomes in Patients with Acute Decompensated Heart Failure with or without Elevated BUN
- PMID: 26769764
- PMCID: PMC4791821
- DOI: 10.2215/CJN.08210815
eGFR and Outcomes in Patients with Acute Decompensated Heart Failure with or without Elevated BUN
Abstract
Background and objectives: In patients with heart failure, the association of renal dysfunction and BUN levels with outcomes is unclear. The aim of our study was to investigate the association between the eGFR at discharge and outcomes in patients with heart failure with or without an elevated BUN level at discharge.
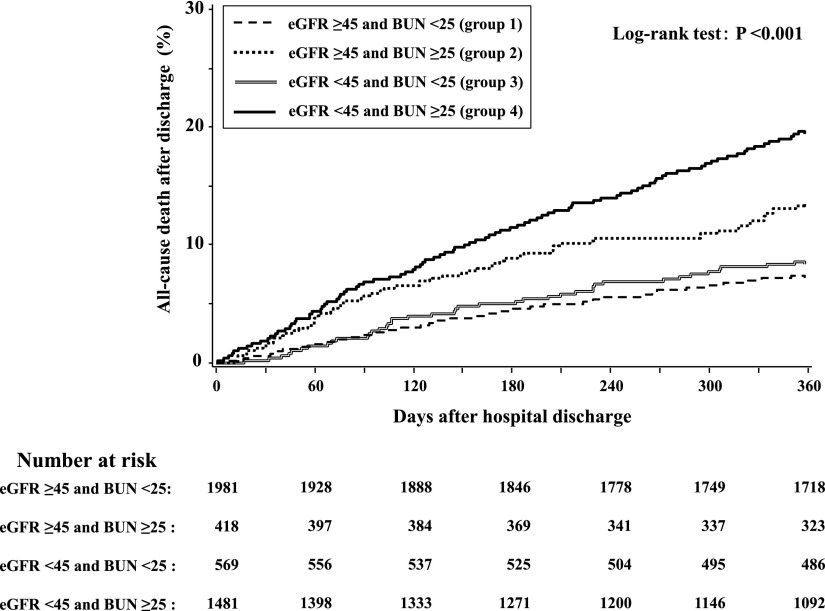
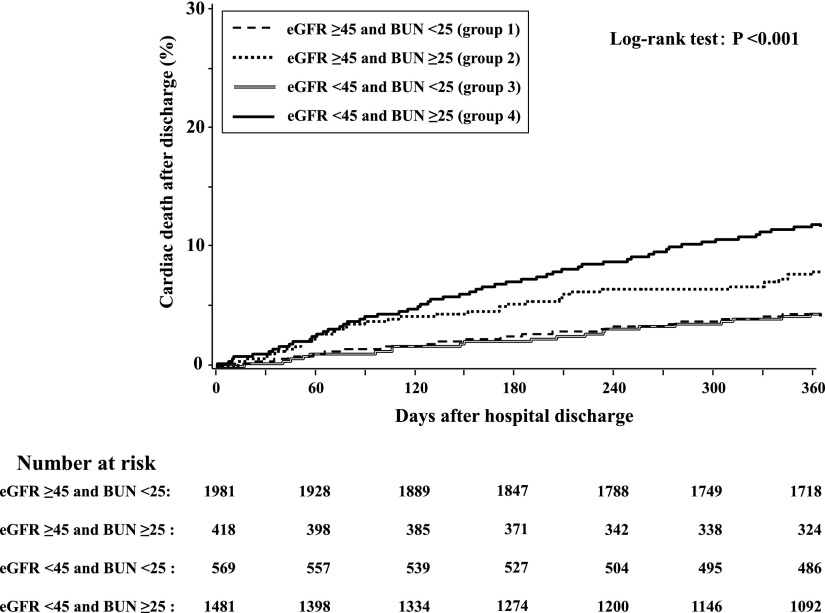
Design, setting, participants, & measurements: Of 4842 patients enrolled in the Acute Decompensated Heart Failure Syndromes Registry, 4449 patients discharged alive after hospitalization for acute decompensated heart failure were investigated to assess the association of eGFR in the context of serum BUN level at discharge with all-cause mortality. The enrolled patients were divided into four groups on the basis of the discharge levels of eGFR (<45 or ≥45 ml/min per 1.73 m(2)) and BUN (≥25 or <25 mg/dl). The median follow-up period after discharge was 517 (381-776) days.
Results: The all-cause mortality rate after discharge was 19.1%. After adjustment for multiple comorbidities, an eGFR<45 ml/min per 1.73 m(2) was associated with a significantly higher risk of all-cause mortality in patients with a BUN≥25 mg/dl (hazard ratio, 1.58; 95% confidence interval, 1.33 to 1.88; P<0.001) but not in patients with a BUN<25 mg/dl (hazard ratio, 0.97; 95% confidence interval, 0.76 to 1.26; P=0.84) relative to those with an eGFR≥45 ml/min per 1.73 m(2) and a BUN<25 mg/dl. Among patients with an eGFR≥45 ml/min per 1.73 m(2), a BUN≥25 mg/dl was associated with a significantly higher risk of all-cause mortality than a BUN<25 mg/dl (hazard ratio, 1.34; 95% confidence interval, 1.04 to 1.73; P=0.02).
Conclusions: We showed that elevation of BUN at discharge significantly modified the relation between eGFR at discharge and the risk of all-cause mortality after discharge, suggesting that the association between eGFR and outcomes may be largely dependent on concomitant elevation of BUN.
Keywords: Comorbidity; Follow-Up Studies; Humans; Patient Discharge; Registries; blood urea nitrogen; glomerular filtration rate; heart failure; hospitalization; outcomes assessment.
Copyright © 2016 by the American Society of Nephrology.
Figures

References
-
- Schrier RW: Role of diminished renal function in cardiovascular mortality: Marker or pathogenetic factor? J Am Coll Cardiol 47: 1–8, 2006 - PubMed
-
- Smith GL, Shlipak MG, Havranek EP, Foody JM, Masoudi FA, Rathore SS, Krumholz HM: Serum urea nitrogen, creatinine, and estimators of renal function: Mortality in older patients with cardiovascular disease. Arch Intern Med 166: 1134–1142, 2006 - PubMed
-
- Smith GL, Lichtman JH, Bracken MB, Shlipak MG, Phillips CO, DiCapua P, Krumholz HM: Renal impairment and outcomes in heart failure: Systematic review and meta-analysis. J Am Coll Cardiol 47: 1987–1996, 2006 - PubMed
-
- Ronco C, Haapio M, House AA, Anavekar N, Bellomo R: Cardiorenal syndrome. J Am Coll Cardiol 52: 1527–1539, 2008 - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
