

The Cost to Successfully Apply for Level 3 Medical Home Recognition
- PMID: 26769879
- PMCID: PMC4878853
- DOI: 10.3122/jabfm.2016.01.150211
The Cost to Successfully Apply for Level 3 Medical Home Recognition
Abstract
Background: The National Committee for Quality Assurance patient-centered medical home recognition program provides practices an opportunity to implement medical home activities. Understanding the costs to apply for recognition may enable practices to plan their work.
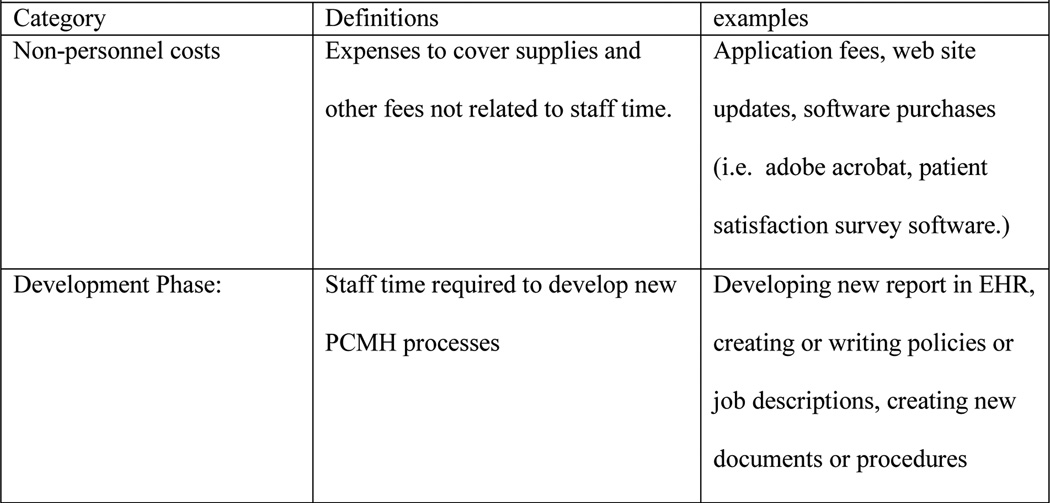
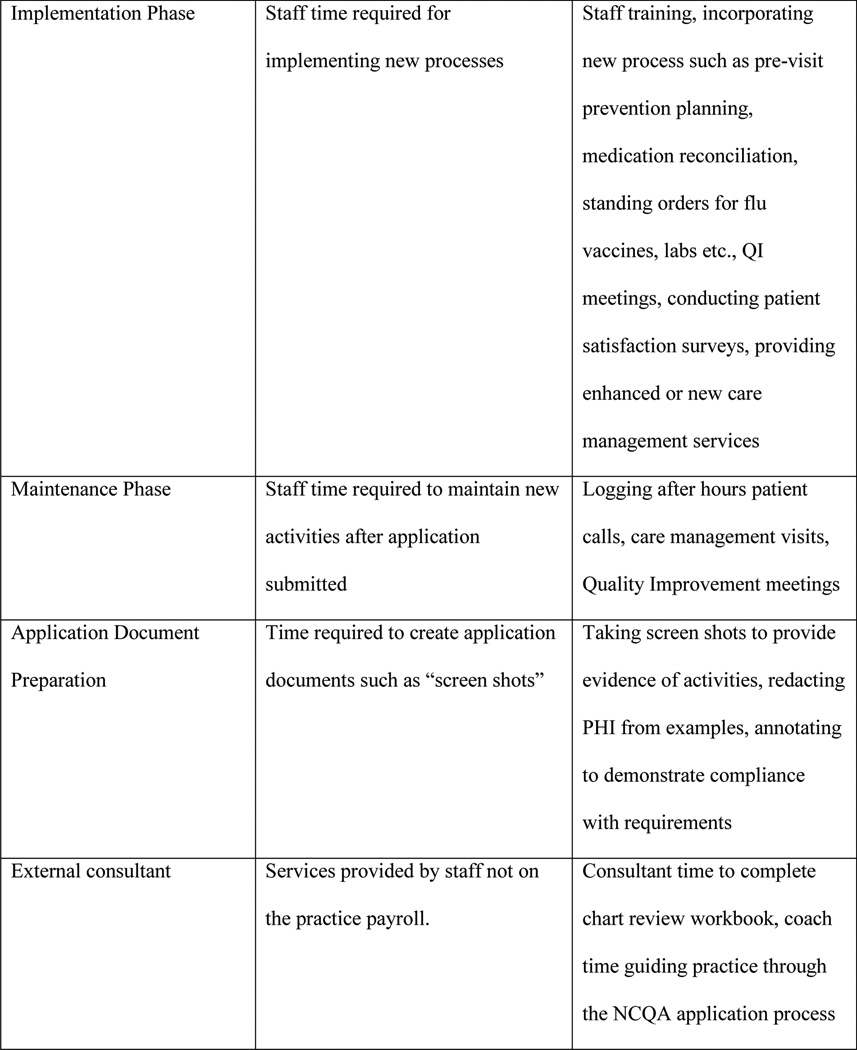
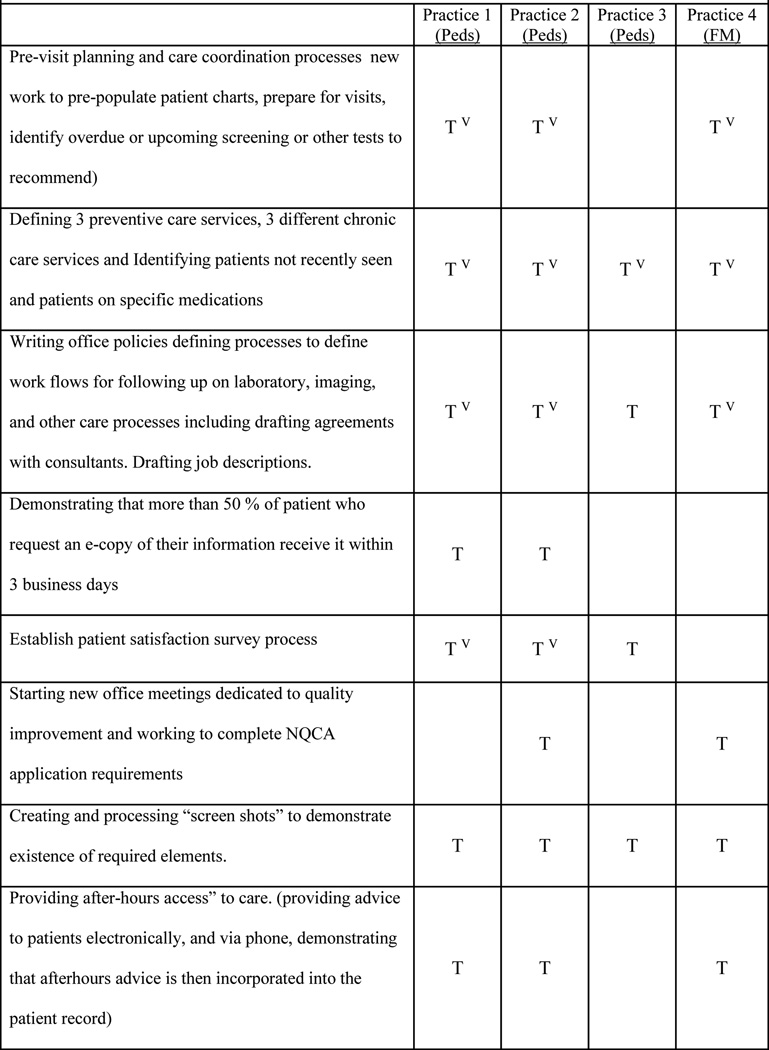
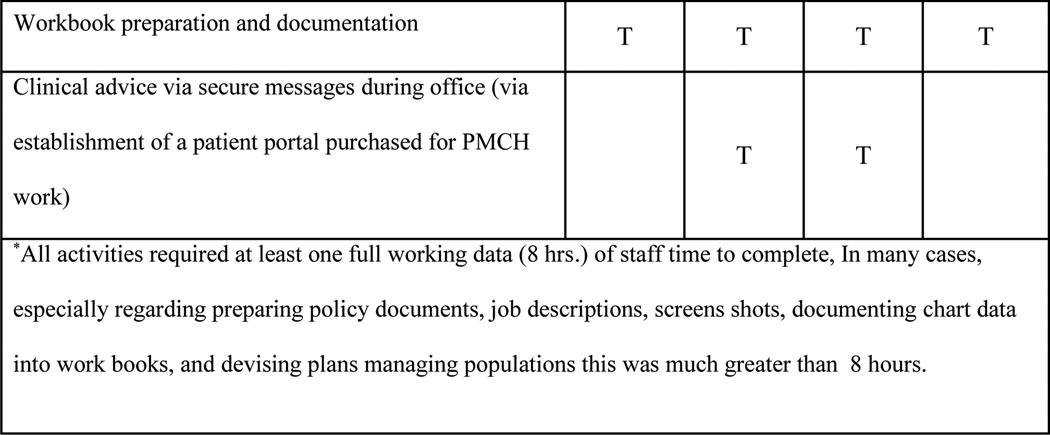
Methods: Practice coaches identified 5 exemplar practices (3 pediatric and 2 family medicine practices) that received level 3 recognition. This analysis focuses on 4 that received recognition in 2011. Clinical, informatics, and administrative staff participated in 2- to 3-hour interviews. We determined the time required to develop, implement, and maintain required activities. We categorized costs as (1) nonpersonnel, (2) developmental, (3) those used to implement activities, (4) those used to maintain activities, (5) those to document the work, and (6) consultant costs. Only incremental costs were included and are presented as costs per full-time equivalent (pFTE) provider.
Results: Practice size ranged from 2.5 to 10.5 pFTE providers, and payer mixes ranged from 7% to 43% Medicaid. There was variation in the distribution of costs by activity by practice, but the costs to apply were remarkably similar ($11,453-15,977 pFTE provider).
Conclusion: The costs to apply for 2011 recognition were noteworthy. Work to enhance care coordination and close loops were highly valued. Financial incentives were key motivators. Future efforts to minimize the burden of low-value activities could benefit practices.
Keywords: Cost Control; Medical Home; Patient-centered Care; Practice Management.
© Copyright 2016 by the American Board of Family Medicine.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Nielson M, Grundy P, Langner B, Zeemer C. Benefits of implementing the primary care patient centered medical home: a review of cost & quality results. [Accessed June, 2015];2012 https://www.pcpcc.org/guide/benefits-implementing-primary-care-medical-home.
-
- Patel MS, Arron MJ, Sinsky TA, et al. Estimating the staffing infrastructure for a patient-centered medical home. The American journal of managed care. 2013 Jun;19(6):509–516. - PubMed
-
- Paulus RA, Davis K, Steele GD. Continuous innovation in health care: implications of the Geisinger experience. Health affairs. 2008 Sep-Oct;27(5):1235–1245. - PubMed
-
- Steele GD, Haynes JA, Davis DE, et al. How Geisinger's advanced medical home model argues the case for rapid-cycle innovation. Health affairs. 2010 Nov;29(11):2047–2053. - PubMed
-
- Fields D, Leshen E, Patel K. Analysis & commentary. Driving quality gains and cost savings through adoption of medical homes. Health affairs. 2010 May;29(5):819–826. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources