

Comprehensive review on endonasal endoscopic sinus surgery
- PMID: 26770282
- PMCID: PMC4702057
- DOI: 10.3205/cto000123
Comprehensive review on endonasal endoscopic sinus surgery
Abstract
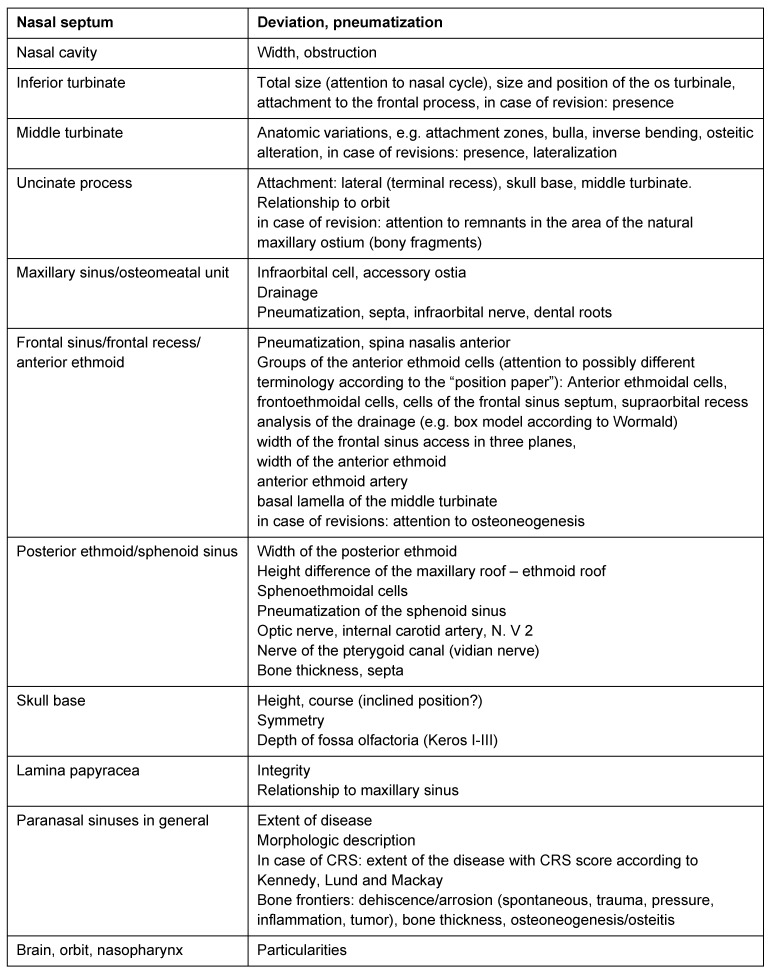
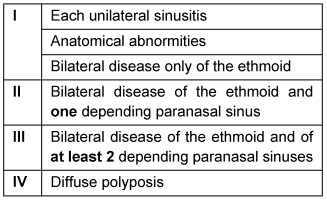
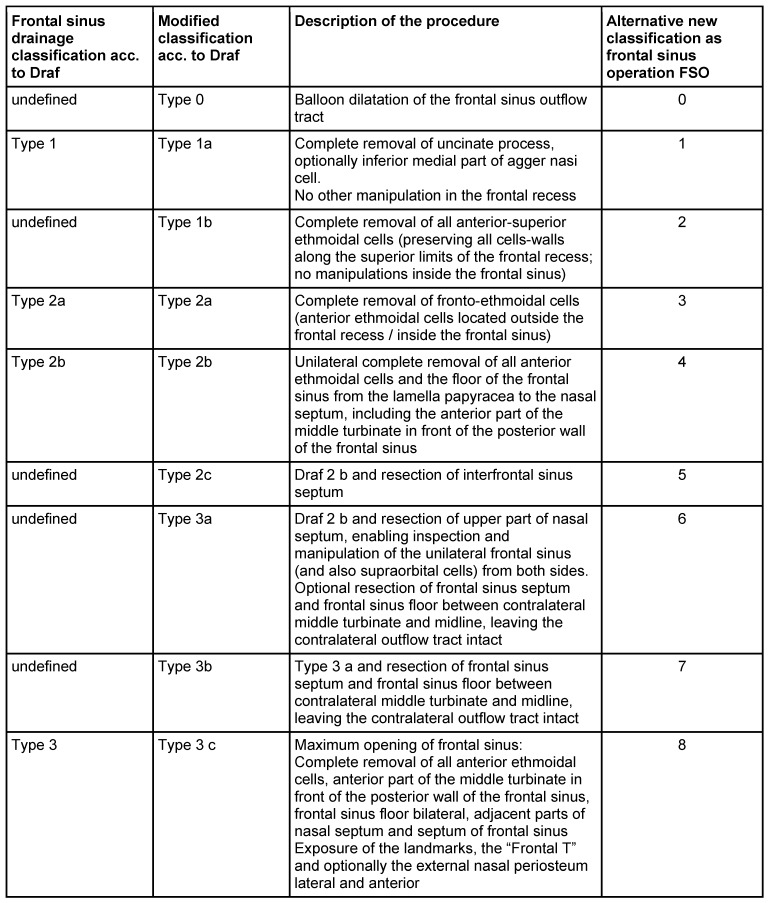
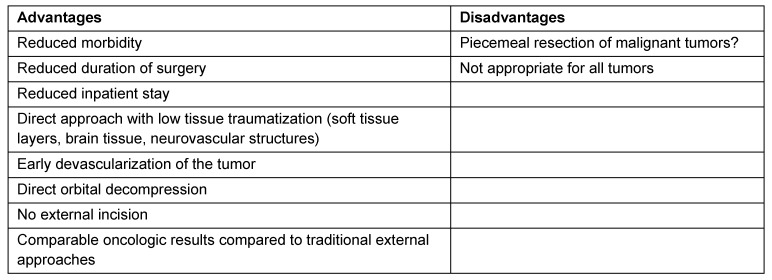
Endonasal endoscopic sinus surgery is the standard procedure for surgery of most paranasal sinus diseases. Appropriate frame conditions provided, the respective procedures are safe and successful. These prerequisites encompass appropriate technical equipment, anatomical oriented surgical technique, proper patient selection, and individually adapted extent of surgery. The range of endonasal sinus operations has dramatically increased during the last 20 years and reaches from partial uncinectomy to pansinus surgery with extended surgery of the frontal (Draf type III), maxillary (grade 3-4, medial maxillectomy, prelacrimal approach) and sphenoid sinus. In addition there are operations outside and beyond the paranasal sinuses. The development of surgical technique is still constantly evolving. This article gives a comprehensive review on the most recent state of the art in endoscopic sinus surgery according to the literature with the following aspects: principles and fundamentals, surgical techniques, indications, outcome, postoperative care, nasal packing and stents, technical equipment.
Keywords: FESS; endoscopic sinus surgery; nasal packing; outcome after sinus surgery; postoperative care after sinus surgery.
Figures





References
-
- Draf W. Die chirurgische Behandlung entzündlicher Erkrankungen der Nasennebenhöhlen. Indikation, Operationsverfahren, Gefahren, Fehler und Komplikationen, Revisionschirurgie. [Surgical treatment of the inflammatory diseases of the paranasal sinuses. Indication, surgical technique, risks, mismanagement and complications, revision surgery]. Arch Otorhinolaryngol. 1982;235(1):133–305. (Ger). - PubMed
-
- Hosemann W. Die endonasale Chirurgie der Nasennebenhöhlen – Konzepte, Techniken, Ergebnisse, Komplikationen, Revisionseingriffe. [Endonasal surgery of the paranasal sinuses - concepts, techniques, results, complications and revision interventions]. Eur Arch Otorhinolaryngol Suppl. 1996;1:155–269. (Ger). - PubMed
-
- Stuck BA, Bachert C, Federspil P, Hosemann W, Klimek L, Mösges R, Pfaar O, Rudack C, Sitter H, Wagenmann M, Weber R, Hörmann K German Society of Otorhinolaryngology, Head and Neck Surgery. Leitlinie "Rhinosinusitis" - Langfassung: S2-Leitlinie der Deutschen Gesellschaft für Hals-Nasen-Ohren-Heilkunde, Kopf- und Hals-Chirurgie. [Rhinosinusitis guidelines - unabridged version: S2 guidelines from the German Society of Otorhinolaryngology, Head and Neck Surgery]. HNO. 2012 Feb;60(2):141–162. doi: 10.1007/s00106-011-2396-7. (Ger). Available from: http://dx.doi.org/10.1007/s00106-011-2396-7. - DOI - PubMed
-
- Hosemann W, Schroeder HW. Comprehensive review on rhino-neurosurgery. GMS Curr Top Otorhinolaryngol Head Neck Surg. 2015;14:Doc01. doi: 10.3205/cto000116. Available from: http://dx.doi.org/10.3205/cto000116. - DOI - PMC - PubMed
-
- Kühnel TS, Reichert TE. Trauma of the midface. GMS Curr Top Otorhinolaryngol Head Neck Surg. 2015;14:Doc06. doi: 10.3205/cto000121. Available from: http://dx.doi.org/10.3205/cto000121. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
