

Reducing the length of postnatal hospital stay: implications for cost and quality of care
- PMID: 26772389
- PMCID: PMC4714454
- DOI: 10.1186/s12913-015-1214-4
Reducing the length of postnatal hospital stay: implications for cost and quality of care
Abstract
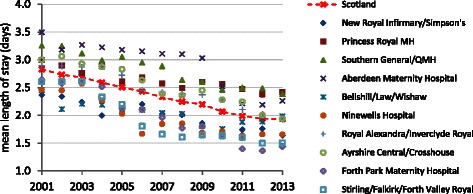
Background: UK health services are under pressure to make cost savings while maintaining quality of care. Typically reducing the length of time patients stay in hospital and increasing bed occupancy are advocated to achieve service efficiency. Around 800,000 women give birth in the UK each year making maternity care a high volume, high cost service. Although average length of stay on the postnatal ward has fallen substantially over the years there is pressure to make still further reductions. This paper explores and discusses the possible cost savings of further reductions in length of stay, the consequences for postnatal services in the community, and the impact on quality of care.
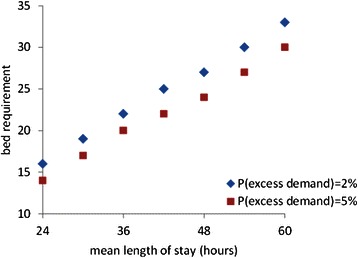
Method: We draw on a range of pre-existing data sources including, national level routinely collected data, workforce planning data and data from national surveys of women's experience. Simulation and a financial model were used to estimate excess demand, work intensity and bed occupancy to explore the quantitative, organisational consequences of reducing the length of stay. These data are discussed in relation to findings of national surveys to draw inferences about potential impacts on cost and quality of care.
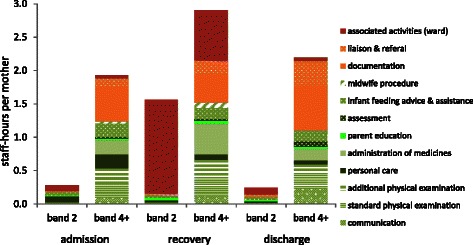
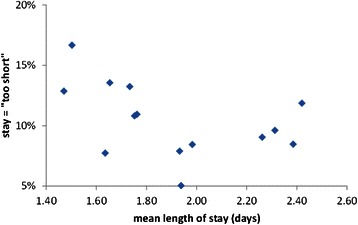
Discursive analysis: Reducing the length of time women spend in hospital after birth implies that staff and bed numbers can be reduced. However, the cost savings may be reduced if quality and access to services are maintained. Admission and discharge procedures are relatively fixed and involve high cost, trained staff time. Furthermore, it is important to retain a sufficient bed contingency capacity to ensure a reasonable level of service. If quality of care is maintained, staffing and bed capacity cannot be simply reduced proportionately: reducing average length of stay on a typical postnatal ward by six hours or 17% would reduce costs by just 8%. This might still be a significant saving over a high volume service however, earlier discharge results in more women and babies with significant care needs at home. Quality and safety of care would also require corresponding increases in community based postnatal care. Simply reducing staffing in proportion to the length of stay increases the workload for each staff member resulting in poorer quality of care and increased staff stress.
Conclusions: Many policy debates, such as that about the length of postnatal hospital-stay, demand consideration of multiple dimensions. This paper demonstrates how diverse data sources and techniques can be integrated to provide a more holistic analysis. Our study suggests that while earlier discharge from the postnatal ward may achievable, it may not generate all of the anticipated cost savings. Some useful savings may be realised but if staff and bed capacity are simply reduced in proportion to the length of stay, care quality may be compromised.
Figures
References
-
- Roberts A, Marshall L, Charlesworth A. A decade of austerity? The funding pressures facing the NHS from 2010/11 to 2021/22. London: Nuffield Trust; 2012.
-
- Monitor. Closing the NHS Funding Gap: how to get better value health care for patients. 2013. https://www.gov.uk/government/publications/closing-the-nhs-funding-gap-h...
-
- National Audit Office. Maternity services in England. 2013. http://www.nao.org.uk/wp-content/uploads/2013/11/10259-001-Maternity-Ser...
-
- Department of Health. Maternity PbR Pathway Payment System 2012–13: Commissioning Maternity Services. 2012. https://www.gov.uk/government/uploads/system/uploads/attachment_data/fil.... Accessed 4th Feb 2015.
-
- NICE National Institute for health and Care Excellence. Maternity Services.https://www.nice.org.uk/guidance/service-delivery--organisation-and-staf.... 2014. Accessed 4 Feb 2015.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
