

The association of serum procalcitonin and high-sensitivity C-reactive protein with pneumonia in elderly multimorbid patients with respiratory symptoms: retrospective cohort study
- PMID: 26772604
- PMCID: PMC4715290
- DOI: 10.1186/s12877-016-0192-7
The association of serum procalcitonin and high-sensitivity C-reactive protein with pneumonia in elderly multimorbid patients with respiratory symptoms: retrospective cohort study
Abstract
Background: Serum procalcitonin and high-sensitivity C-reactive protein (hs-CRP) elevations have been associated with pneumonia in adults. Our aim was to establish their diagnostic usefulness in a cohort of hospitalized multimorbid patients ≥65 years old admitted to hospital with acute respiratory symptoms.
Methods: With a retrospective cohort study design, all multimorbid patients ≥65 years-old with acute respiratory symptoms admitted to an internal medicine hospital ward in Italy from January to August 2013 were evaluated. Pneumonia diagnosis, comorbidities expressed through Cumulative Illness Rating Scale (CIRS), setting of living, length of stay, serum hs-CRP and procalcitonin at admission were collected for each patient. Data were analyzed with Mann-Whitney's U test and multivariate Cox logistic regression analysis. A Receiver Operating Characteristic (ROC) curve was used to verify each biomarker's association with pneumonia diagnosis.
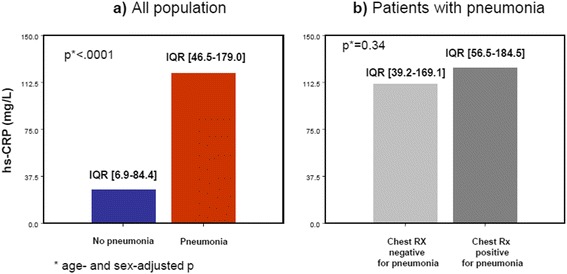
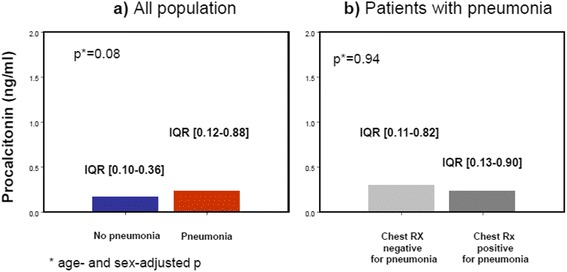
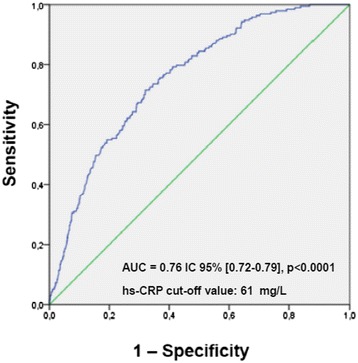
Results: Four hundred fifty five patients (227 M) were included in the study, of whom 239 with pneumonia (138 M, mean age 80 ± 13) and 216 without pneumonia (89 M, mean age 80 ± 14). After adjustment for age and sex, median levels of hs-CRP were significantly higher in patients with pneumonia (116 mg/L, IQR 46.5-179.0, vs 22.5 mg/dl, IQR 6.9-84.4, p < 0.0001), while procalcitonin median levels were not (0.22 ng/ml IQR 0.12-0.87, vs 0.15 ng/ml, IQR 0.10-0.35, p = 0.08). The ROC analysis showed that, unlike procalcitonin, hs-CRP values were predictive of pneumonia (AUC 0.76, 95% CI 0.72-0.79, p < 0.0001, cut-off value 61 mg/L), even after adjustment for possible confounders including nursing home residence and dementia. Serum hs-CRP levels >61 mg/L were independently associated with a 3.59-fold increased risk of pneumonia (OR 3.59, 95% CI 2.35-5.48, p < 0.0001).
Conclusion: In elderly multimorbid patients who require hospital admission for respiratory symptoms, serum hs-CRP testing seems to be more useful than procalcitonin for guiding the diagnostic process when clinical suspicion of pneumonia is present. Procalcitonin testing might hence be not recommended in this setting.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
