

Outcomes of Adjuvant Mitotane after Resection of Adrenocortical Carcinoma: A 13-Institution Study by the US Adrenocortical Carcinoma Group
- PMID: 26775162
- PMCID: PMC4957938
- DOI: 10.1016/j.jamcollsurg.2015.12.013
Outcomes of Adjuvant Mitotane after Resection of Adrenocortical Carcinoma: A 13-Institution Study by the US Adrenocortical Carcinoma Group
Erratum in
-
Correction.J Am Coll Surg. 2018 Jan;226(1):114. doi: 10.1016/j.jamcollsurg.2017.09.011. J Am Coll Surg. 2018. PMID: 29274650 No abstract available.
Abstract
Background: Current treatment guidelines recommend adjuvant mitotane after resection of adrenocortical carcinoma with high-risk features (eg, tumor rupture, positive margins, positive lymph nodes, high grade, elevated mitotic index, and advanced stage). Limited data exist on the outcomes associated with these practice guidelines.
Study design: Patients who underwent resection of adrenocortical carcinoma from 1993 to 2014 at the 13 academic institutions of the US Adrenocortical Carcinoma Group were included. Factors associated with mitotane administration were determined. Primary end points were recurrence-free survival (RFS) and overall survival (OS).
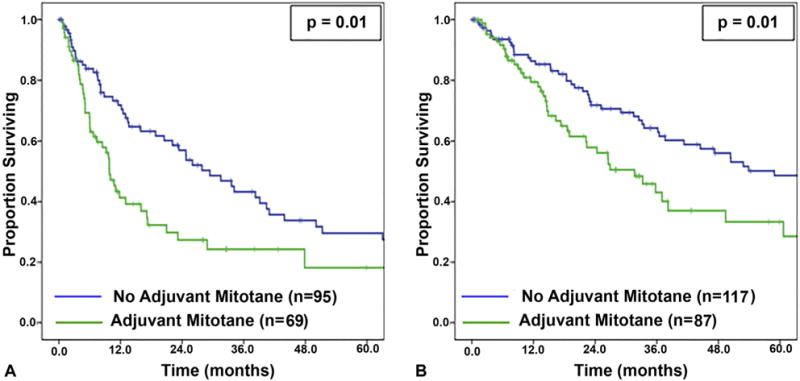
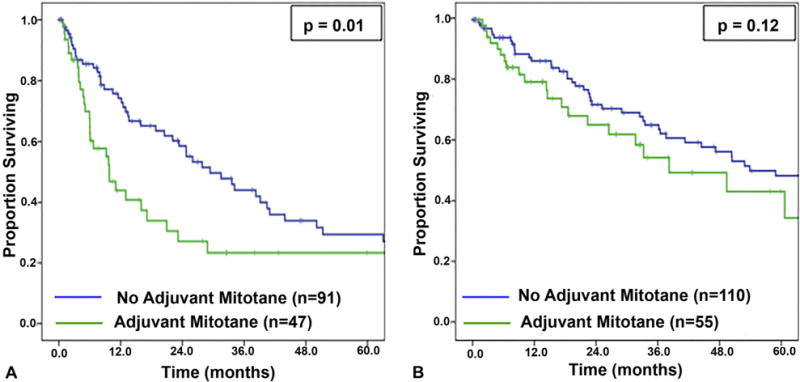
Results: Of 207 patients, 88 (43%) received adjuvant mitotane. Receipt of mitotane was associated with hormonal secretion (58% vs 32%; p = 0.001), advanced TNM stage (stage IV: 42% vs 23%; p = 0.021), adjuvant chemotherapy (37% vs 5%; p < 0.001), and adjuvant radiation (17% vs 5%; p = 0.01), but was not associated with tumor rupture, margin status, or N-stage. Median follow-up was 44 months. Adjuvant mitotane was associated with decreased RFS (10.0 vs 27.9 months; p = 0.007) and OS (31.7 vs 58.9 months; p = 0.006). On multivariable analysis, mitotane was not independently associated with RFS or OS, and margin status, advanced TNM stage, and receipt of chemotherapy were associated with survival. After excluding all patients who received chemotherapy, adjuvant mitotane remained associated with decreased RFS and similar OS; multivariable analyses again showed no association with recurrence or survival. Stage-specific analyses in both cohorts revealed no association between adjuvant mitotane and improved RFS or OS.
Conclusions: When accounting for stage and adverse tumor and treatment-related factors, adjuvant mitotane after resection of adrenocortical carcinoma is not associated with improved RFS or OS. Current guidelines should be revisited and prospective trials are needed.
Copyright © 2016 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Discussion.J Am Coll Surg. 2016 Apr;222(4):490-2. doi: 10.1016/j.jamcollsurg.2016.01.031. J Am Coll Surg. 2016. PMID: 27016977 No abstract available.
-
[Adjuvant mitotane treatment after adrenalectomy is not beneficial for adrenocortical carcinoma].Chirurg. 2016 Nov;87(11):980. doi: 10.1007/s00104-016-0288-9. Chirurg. 2016. PMID: 27604235 German. No abstract available.
References
-
- Kebebew E, Reiff E, Duh QY, et al. Extent of disease at presentation and outcome for adrenocortical carcinoma: have we made progress? World J Surg. 2006;30:872–878. - PubMed
-
- Schulick RD, Brennan MF. Long-term survival after complete resection and repeat resection in patients with adrenocortical carcinoma. Ann Surg Oncol. 1999;6:719–726. - PubMed
-
- Bilimoria KY, Shen WT, Elaraj D, et al. Adrenocortical carcinoma in the United States: treatment utilization and prognostic factors. Cancer. 2008;113:3130–3136. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
