

[Ability to detect psychiatric disorders by the family physician]
- PMID: 26775265
- PMCID: PMC6877835
- DOI: 10.1016/j.aprim.2015.09.009
[Ability to detect psychiatric disorders by the family physician]
Abstract
Objective: To determine the ability of family physicians to detect psychiatric disorders, comparing the presence of psychiatric disorders detected using validated tests and referrals by family physicians.
Design: Cross-sectional, two-phase study.
Location: Primary healthcare centres in an urban area of Madrid.
Participants: Patients between 18 and 65years attending primary healthcare centres for non-administrative purposes.
Main measurements: To detect psychiatric disorders in the waiting room, an interview was performed using GHQ-28 and MULTICAGE CAD-4 in the screening phase (considered positive: score of 6 or higher on the GHQ-28 or a score 2 or higher on MULTICAGE CAD-4). Patients with a positive score and 20% with negative were recruited for the second phase (case identification) using MINI interview. During family physician consultation, the patient gave his doctor a card with an identification number to record the presence of psychiatric illness in his/her opinion and whether there was treatment with psychotropic drugs.
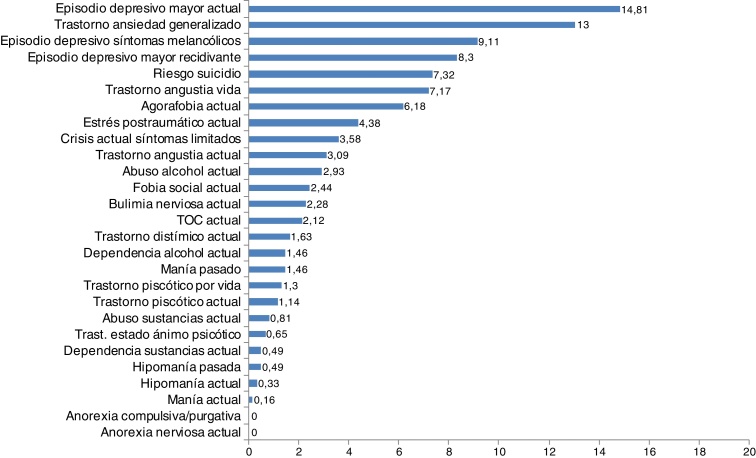
Results: A total of 628 subjects participated. The prevalence of psychiatric disorders corrected by two phase methodology was 31.7% (95%CI: 27.9 to 35.5). Of the 185 patients with a psychiatric disorder detected, 44.2% (95%CI: 36.7 to 51.7) were identified as patients with psychiatric disorders by their family physician. Disorders best detected were: hypomania, dysthymic disorder, depressive episode with melancholic symptoms, and panic disorder.
Conclusions: A significant percentage of patients with possible psychiatric disorders detected with validated test have not been identified by their family physician.
Objetivo: Conocer la capacidad de detección de patología psiquiátrica por el médico de familia, comparando la presencia de patología psiquiátrica detectada mediante test validados y la referida por su médico de familia.
Diseño: Estudio transversal de doble fase.
Emplazamiento: Centros de Salud de un área urbana de Madrid.
Participantes: Pacientes entre 18 y 65 años que acuden a consulta por motivos no administrativos.
Mediciones principales: Para la detección de posible patología psiquiátrica, en la sala de espera se utilizaron instrumentos de cribado, el GHQ-28 (punto de corte 6 o superior) y el MULTICAGE CAD-4 (punto de corte 2 o superior). Como instrumento de identificación de «caso» en la segunda fase se utilizó la entrevista MINI en los pacientes con puntuación positiva en uno de los instrumentos de cribado y un 20% de los negativos. Por otro lado, cuando los pacientes entraban en la consulta entregaban a su médico una tarjeta con un número de identificación para que, de manera ciega, registrase: presencia de patología psiquiátrica actual según su criterio y existencia, o no, de tratamiento actual con psicofármacos.
Resultados: Participaron 628 sujetos. La prevalencia de patología psiquiátrica corregida por metodología de doble fase fue del 31,7% (IC 95%: 27,9-35,5). De 185 pacientes con patología psiquiátrica detectada, el 44,2% (IC 95%: 36,7-51,7) fueron identificados como pacientes con patología psiquiátrica por su médico de familia. Las patologías mejor identificadas fueron: hipomanía, trastorno distímico, episodio depresivo con síntomas melancólicos y trastorno por angustia.
Conclusiones: Un porcentaje importante de pacientes con patología psiquiátrica detectada con test validados no han sido identificados por su médico de familia.
Keywords: Atención primaria; Habilidad diagnóstica; Patología psiquiátrica; Primary care; Psychiatric disorder; Recognition.
Copyright © 2015 Elsevier España, S.L.U. All rights reserved.
Figures
Similar articles
-
[Prevalence of psychiatric disorders in French general practice using the patient health questionnaire: comparison with GP case-recognition and psychotropic medication prescription].Encephale. 2009 Dec;35(6):560-9. doi: 10.1016/j.encep.2008.06.018. Encephale. 2009. PMID: 20004287 French.
-
Psychiatric morbidity and predisposing factors in a primary care population in Madrid.Int J Soc Psychiatry. 2015 May;61(3):275-86. doi: 10.1177/0020764014542815. Epub 2014 Jul 24. Int J Soc Psychiatry. 2015. PMID: 25063751
-
Prevalence, recognition and management of mental disorders in primary health care in Northern Jordan.Acta Psychiatr Scand. 1997 Jul;96(1):31-5. doi: 10.1111/j.1600-0447.1997.tb09901.x. Acta Psychiatr Scand. 1997. PMID: 9259221
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) acute day hospital versus admission; (2) vocational rehabilitation; (3) day hospital versus outpatient care.Health Technol Assess. 2001;5(21):1-75. doi: 10.3310/hta5210. Health Technol Assess. 2001. PMID: 11532238 Review.
-
Psychiatric consultation and referral.Med Clin North Am. 1988 Jul;72(4):929-35. doi: 10.1016/s0025-7125(16)30753-2. Med Clin North Am. 1988. PMID: 3287044 Review.
Cited by
-
Increased Risks of Mental Disorders: Youth with Inactive Physical Activity.Healthcare (Basel). 2022 Jan 26;10(2):237. doi: 10.3390/healthcare10020237. Healthcare (Basel). 2022. PMID: 35206852 Free PMC article.
-
[Translation and cross-cultural adaptation into Spanish, Catalan and Galician of the Hopkins Symptom Checklist-25 to identify depression in Primary Care].Aten Primaria. 2020 Oct;52(8):539-547. doi: 10.1016/j.aprim.2020.05.017. Epub 2020 Jul 20. Aten Primaria. 2020. PMID: 32703629 Free PMC article. Spanish.
-
Measuring depression in Primary Health Care in Spain: Psychometric properties and diagnostic accuracy of HSCL-5 and HSCL-10.Front Med (Lausanne). 2023 Jan 9;9:1014340. doi: 10.3389/fmed.2022.1014340. eCollection 2022. Front Med (Lausanne). 2023. PMID: 36698836 Free PMC article.
-
[Comment to the article «The hability of family doctor detecting psychiatric pathology»].Aten Primaria. 2017 Aug-Sep;49(7):440-441. doi: 10.1016/j.aprim.2016.11.009. Epub 2017 Apr 10. Aten Primaria. 2017. PMID: 28408114 Free PMC article. Spanish. No abstract available.
-
Multimorbid outpatients: A high frequency of FP appointments and/or family difficulties, should alert FPs to the possibility of death or acute hospitalization occurring within six months; A primary care feasibility study.PLoS One. 2017 Nov 2;12(11):e0186931. doi: 10.1371/journal.pone.0186931. eCollection 2017. PLoS One. 2017. PMID: 29095849 Free PMC article.
References
-
- Reneses B., Garrido-Elustondo S., Navalon A., Martin O., Ramos I., Fuentes M. Psychiatric morbidity and predisposing factors in a primary care population in Madrid. Int J Soc Psychiatry. 2015;61:275–286. - PubMed
-
- Norton J., de Roquefeuil G., David M., Boulenger J.P., Ritchie K., Mann A. Prevalence of psychiatric disorders in French general practice using the patient health questionnaire: Comparison with GP case-recognition and psychotropic medication prescription. Encephale. 2009;35:560–569. - PubMed
-
- Ansseau M., Dierick M., Buntinchkx F., Cnoekaert P., de Snedt J., van Den H. High prevalence of mental disorders in primary care. J Affect Disord. 2004;78:48–59. - PubMed
-
- Serrano-Blanco A., Palao D.J., Luciano J.V., Pinto-Meza A., Lujan L., Fernandez A. Prevalence of mental disorders in primary care: Results from the diagnosis and treatment of mental disorders in primary care study (DASMAP) Soc Psychiatry Psychiatr Epidemiol. 2010;45:201–210. - PubMed
-
- Roca M., Gili M., García-García M., Salva J., Vives M., Garcia C. Prevalence and comorbidity of common mental disorders in primary care. J Affect Disord. 2009;119:52–58. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
