

KIDNEY DISEASE GENETICS AND THE IMPORTANCE OF DIVERSITY IN PRECISION MEDICINE
- PMID: 26776194
- PMCID: PMC4720994
KIDNEY DISEASE GENETICS AND THE IMPORTANCE OF DIVERSITY IN PRECISION MEDICINE
Abstract
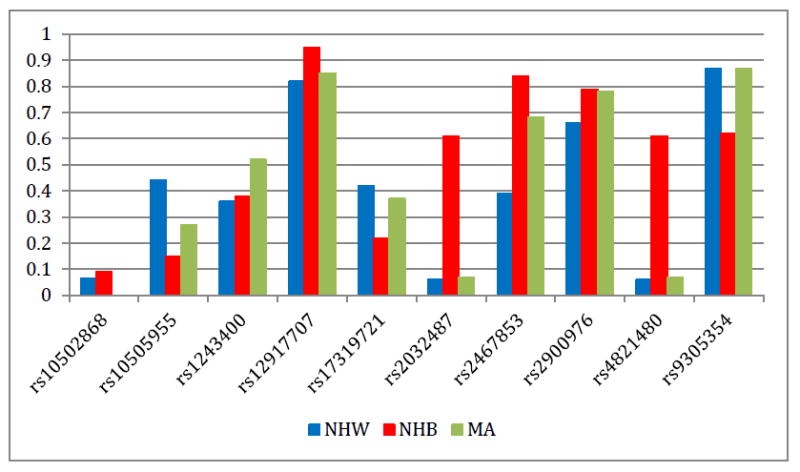
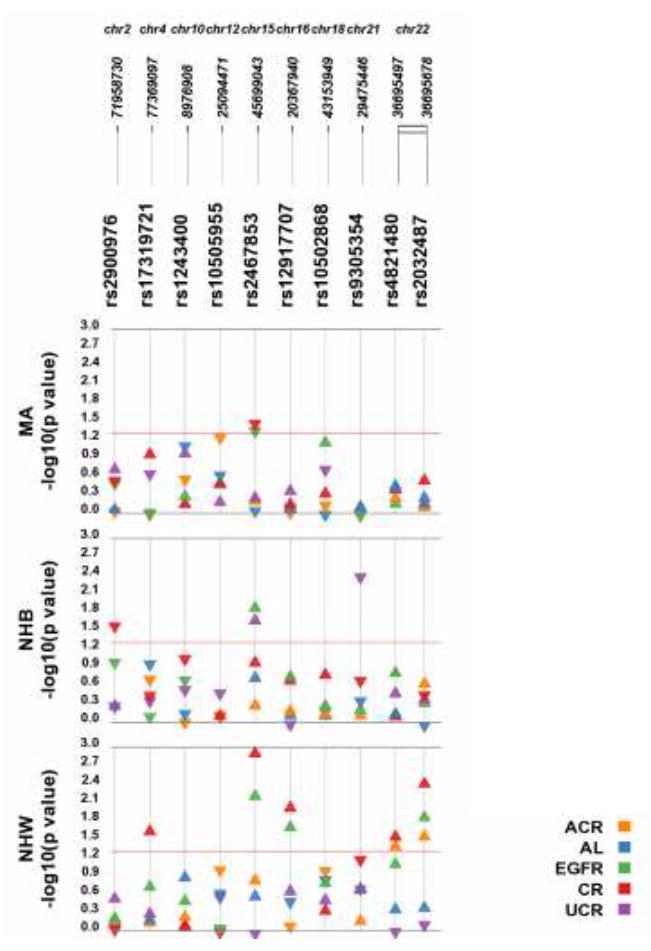
Kidney disease is a well-known health disparity in the United States where African Americans are affected at higher rates compared with other groups such as European Americans and Mexican Americans. Common genetic variants in the myosin, heavy chain 9, non-muscle (MYH9) gene were initially identified as associated with non-diabetic end-stage renal disease in African Americans, and it is now understood that these variants are in strong linkage disequilibrium with likely causal variants in neighboring APOL1. Subsequent genome-wide and candidate gene studies have suggested that MYH9 common variants among others are also associated with chronic kidney disease and quantitative measures of kidney function in various populations. In a precision medicine setting, it is important to consider genetic effects or genetic associations that differ across racial/ethnic groups in delivering data relevant to disease risk or individual-level patient assessment. Kidney disease and quantitative trait-associated genetic variants have yet to be systematically characterized in multiple racial/ethnic groups. Therefore, to further characterize the prevalence of these genetic variants and their association with kidney related traits, we have genotyped 10 kidney disease or quantitative trait-associated single nucleotide polymorphisms (SNPs) (rs2900976, rs10505955, rs10502868, rs1243400, rs9305354, rs12917707, rs17319721, rs2467853, rs2032487, and rs4821480) in 14,998 participants from the population-based cross-sectional National Health and Nutrition Examination Surveys (NHANES) III and 1999-2002 as part of the Epidemiologic Architecture for Genes Linked to Environment (EAGLE) study. In this general adult population ascertained regardless of health status (6,293 non-Hispanic whites, 3,013 non-Hispanic blacks, and 3,542 Mexican Americans), we observed higher rates of chronic kidney disease among non-Hispanic blacks compared with the other groups as expected. We performed single SNP tests of association using linear regressions assuming an additive genetic model adjusted for age, sex, diastolic blood pressure, systolic blood pressure, and type 2 diabetes status for several outcomes including creatinine (urinary), creatinine (serum), albumin (urinary), eGFR, and albumin-to-urinary creatinine ratio (ACR). We also tested for associations between each SNP and chronic kidney disease and albuminuria using logistic regression. Surprisingly, none of the MYH9 variants tested was associated with kidney diseases or traits in non-Hispanic blacks (p>0.05), perhaps attributable to the clinical heterogeneity of kidney disease in this population. Several associations were observed in each racial/ethnic group at p<0.05, but none were consistently associated in the same direction in all three groups. The lack of significant and consistent associations is most likely due to power highlighting the importance of the availability of large, diverse populations for genetic association studies of complex diseases and traits to inform precision medicine efforts in diverse patient populations.
Figures
References
-
- USRDS Coordinating Center. United States Renal Data System. ( www.usrds.org). Accessed July 24, 2015.
-
- Cowie CC, Port FK, Wolfe RA, SAVAGE PJ, Moll PP, Hawthorne VM. Disparities in Incidence of Diabetic End-Stage Renal Disease According to Race and Type of Diabetes. N Engl J Med. 1989;321:1074–1079. - PubMed
-
- Williams WW, Pollak MR. Health Disparities in Kidney Disease--Emerging Data from the Human Genome. N Engl J Med. 2013;369:2260–2261. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
