

Indications for staging laparoscopy in pancreatic cancer
- PMID: 26776846
- PMCID: PMC4750228
- DOI: 10.1016/j.hpb.2015.10.004
Indications for staging laparoscopy in pancreatic cancer
Abstract
Background: To identify indications for staging laparoscopy (SL) in patients with resectable pancreatic cancer, and suggest a pre-operative algorithm for staging these patients.
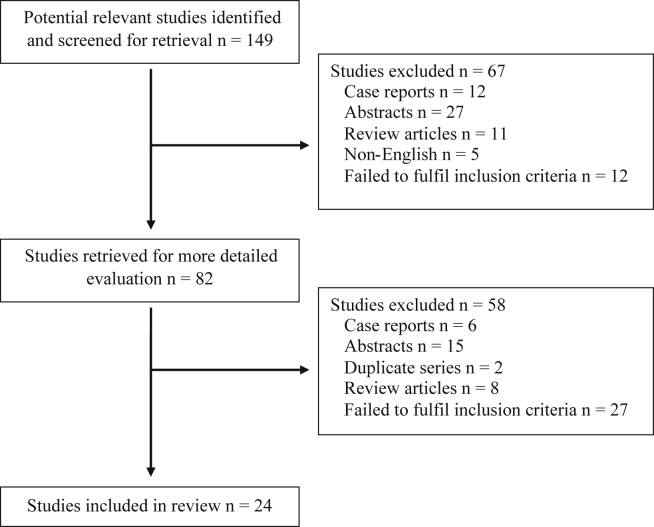
Methods: Relevant articles were reviewed from the published literature using the Medline database. The search was performed using the keywords 'pancreatic cancer', 'resectability', 'staging', 'laparoscopy', and 'Whipple's procedure'.
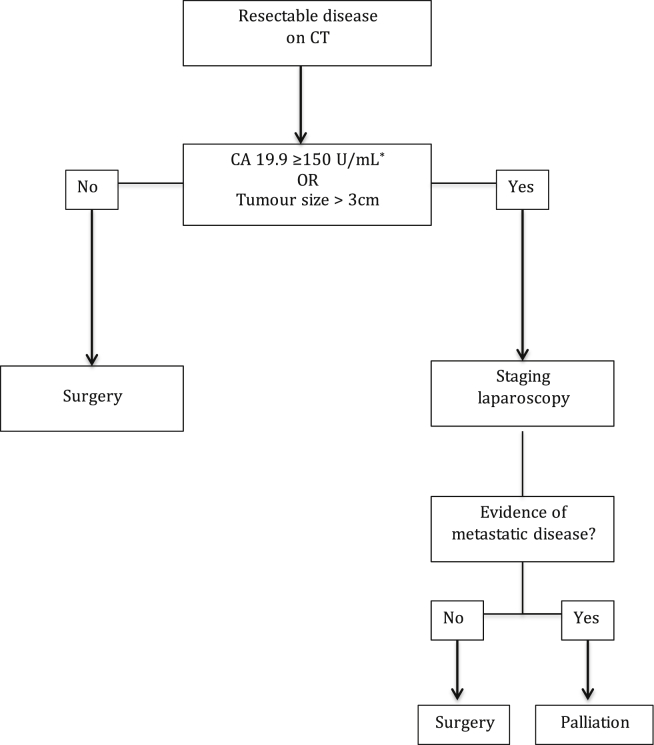
Results: Twenty four studies were identified which fulfilled the inclusion criteria. Of the published data, the most reliable surrogate markers for selecting patients for SL to predict unresectability in patients with CT defined resectable pancreatic cancer were CA 19.9 and tumour size. Although there are studies suggesting a role for tumour location, CEA levels, and clinical findings such as weight loss and jaundice, there is currently not enough evidence for these variables to predict resectability. Based on the current data, patients with a CT suggestive of resectable disease and (1) CA 19.9 ≥150 U/mL; or (2) tumour size >3 cm should be considered for SL.
Conclusion: The role of laparoscopy in the staging of pancreatic cancer patients remains controversial. Potential predictors of unresectability to select patients for SL include CA 19.9 levels and tumour size.
Copyright © 2015 International Hepato-Pancreato-Biliary Association Inc. Published by Elsevier Ltd. All rights reserved.
Figures
References
-
- Takai S., Satoi S., Toyokawa H., Yanagimoto H., Sugimoto N., Tsuji K. Clinicopathologic evaluation after resection for ductal adenocarcinoma of the pancreas: a retrospective, single-institution experience. Pancreas. 2003;26:243–249. - PubMed
-
- Yeo C.J., Cameron J.L., Lillemoe K.D., Sohn T.A., Campbell K.A., Sauter P.K. Pancreaticoduodenectomy with or without distal gastrectomy and extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma, part 2: randomized controlled trial evaluating survival, morbidity, and mortality. Ann Surg. 2002;236:355–366. discussion 366–358. - PMC - PubMed
-
- Pedrazzoli S., DiCarlo V., Dionigi R., Mosca F., Pederzoli P., Pasquali C. Standard versus extended lymphadenectomy associated with pancreatoduodenectomy in the surgical treatment of adenocarcinoma of the head of the pancreas - a multicenter, prospective, randomized study. Ann Surg. 1998;228:508–514. - PMC - PubMed
-
- Bipat S., Phoa S., van Delden O.M., Bossuyt P.M.M., Gouma D.J., Lameris J.S. Ultrasonography, computed tomography and magnetic resonance imaging for diagnosis and determining resectability of pancreatic adenocarcinoma – a meta-analysis. J Comput Assisted Tomogr. 2005;29:438–445. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
