

Fluid collection after distal pancreatectomy: a frequent finding
- PMID: 26776849
- PMCID: PMC4750236
- DOI: 10.1016/j.hpb.2015.10.006
Fluid collection after distal pancreatectomy: a frequent finding
Abstract
Background: Fluid collections (FC) at the resection margin of the pancreatic stump after distal pancreatectomy (DP) are common radiological findings in follow-up scans. No recommendations exist regarding the management of such findings. The aim was to characterise incidence, risk factors, clinical impact and therapy of FC.
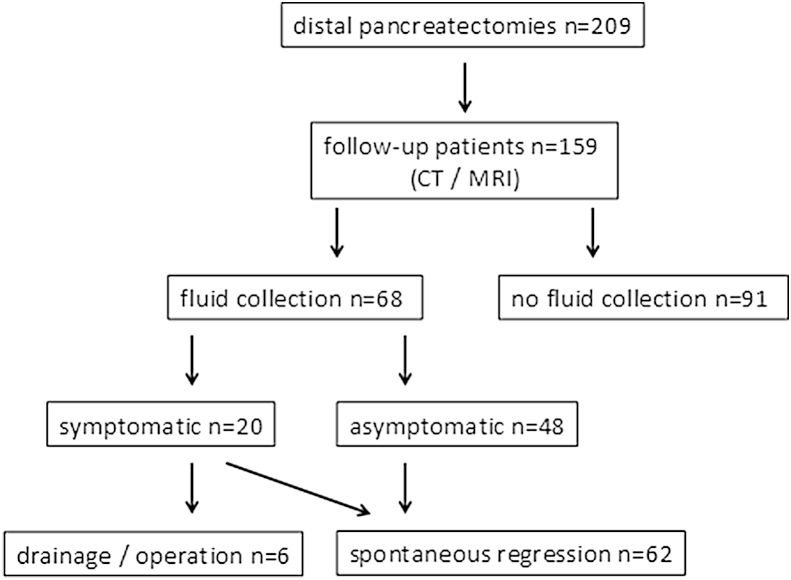
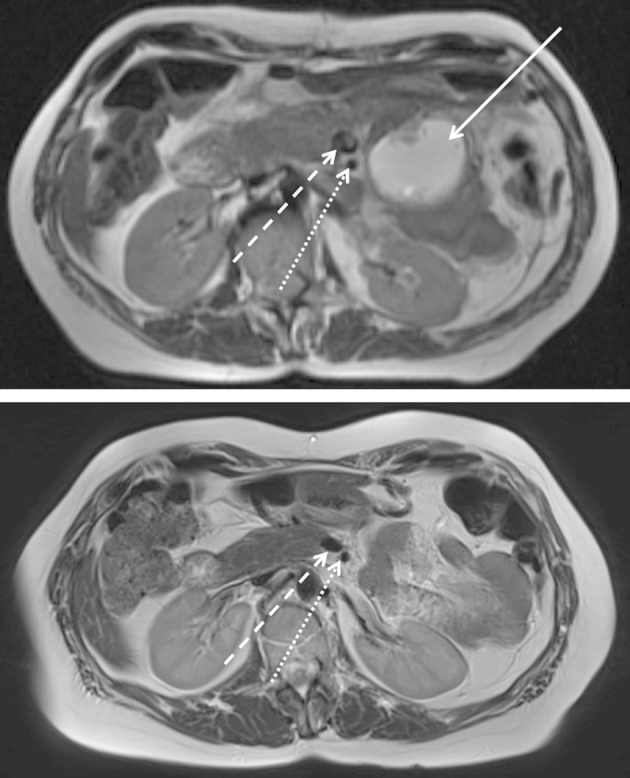
Method: Data of 209 patients who underwent DP between 07/2009 and 06/2011 were prospectively collected and analysed, regarding follow-up CT or MRI scan findings of FC at the resection margin. FC was defined as a cyst-like lesion >1 cm in diameter.
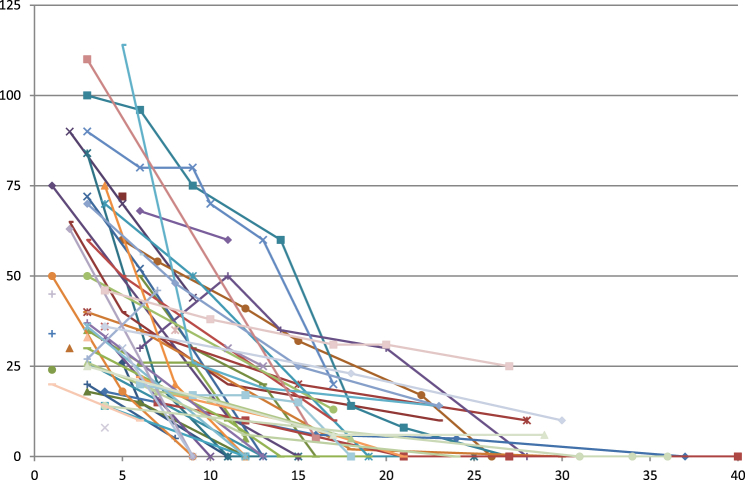
Results: A follow-up with at least two cross-sectional images was available in 159/209 patients. In the first postoperative control, 68 patients showed an FC (43%). FC size was classified as <5 cm (n = 38 pat.), 5-10 cm (n = 24 pat.) and >10 cm (n = 6 pat.). 20 patients (30%) showed clinical symptoms. Six patients (9%) required specific treatment, all other FC showed spontaneous regression. No correlation with stump closure techniques or preceding postoperative pancreatic fistula was found (4/68 patients, 6%). Multivariate analysis revealed standard resections as the only significant factor for FC.
Conclusions: FCs at the resection margin after DP are frequent and harmless findings. Therapeutic interventions are required in only 9% of all FC patients.
Copyright © 2015 International Hepato-Pancreato-Biliary Association Inc. Published by Elsevier Ltd. All rights reserved.
Figures
References
-
- Goh B.K., Tan Y.M., Chung Y.F., Cheow P.C., Ong H.S., Chan W.H. Critical appraisal of 232 consecutive distal pancreatectomies with emphasis on risk factors, outcome, and management of the postoperative pancreatic fistula: a 21-year experience at a single institution. Arch Surg. 2008;143:956–965. - PubMed
-
- Hackert T., Büchler M.W. Remnant closure after distal pancreatectomy: current state and future perspectives. Surgeon. 2012;10:95–101. - PubMed
-
- Diener M.K., Seiler C.M., Rossion I., Kleeff J., Glanemann M., Butturini G. Efficacy of stapler versus hand-sewn closure after distal pancreatectomy (DISPACT): a randomised, controlled multicentre trial. Lancet. 2011;377:1514–1522. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
